Photobiomodulation of Aging Tissues: Optimization of Dosimetric Parameters, Optical Modeling and Biphasic Dose Response
Abstract
Aging is characterized by progressive mitochondrial dysfunction, oxidative stress, chronic inflammation and impaired tissue regeneration, all of which culminate in degenerative conditions and poor healing capacity. Photobiomodulation (PBM), which utilizes red and near-infrared light (600-1000 nm), represents an emerging, non-invasive treatment modality that can be used to regulate cellular processes for maintaining tissue homeostasis. This review aims at providing a thorough overview of PBM with regards to aging, from cell biology to optics and from clinical applications to dosimetry. In terms of cellular biology, PBM involves the absorption of photons by mitochondrial photosensitizers resulting in ATP production stimulation, ROS signaling modulation, as well as activation of signaling cascades responsible for inflammation resolution and tissue repair. Nevertheless, PBM's therapeutic effect is greatly dependent upon optical properties of aging tissues, where light scattering increases along with the change in the chromophore concentration profile affecting light fluence distribution. The biphasic dose–response relationship is of particular interest here, as it demonstrates the presence of the optimal therapeutic window in which photobiomodulation stimulates biological effects, but low and high dosages can fail to work properly. The usage of modern computational techniques like the Monte Carlo simulation of light transport is suggested as a key factor for predicting energy deposition. From a clinical point of view, photobiomodulation shows promise in dealing with chronic wounds, musculoskeletal issues, neurodegenerative diseases and aging of the skin. Generally speaking, this paper focuses on the necessity to combine biophysical and biological knowledge to advance photobiomodulation in geriatric medicine.
Keywords: Aging, Wound healing, Photobiomodulation, Tissue regeneration, Low-level laser therapy, Dosimetry.
1. Introduction
The aging process itself is very complicated biologically and entails the occurrence of deterioration in cellular physiology, decreased regenerative capabilities and increased vulnerability to illnesses and other ailments. Such changes occur as a result of mitochondrial abnormalities, oxidative stress, chronic inflammatory response and decreased reparative properties of tissue structures. These findings indicate that problems such as chronic wounds, joint degeneration, neurodegeneration and skin aging constitute serious issues in contemporary medicine1.
Recent developments in photobiomodulation (PBM), formerly referred to as low-level laser therapy (LLLT), have identified it as a potential non-invasive intervention that involves modulating cellular function to promote tissue regeneration. This form of intervention involves the use of photons from red and near-infrared light ranging from 600–1000 nm to induce photochemical processes within cells, unlike other methods involving heat. On a cellular level, photons are absorbed by mitochondrial chromophores, especially cytochrome c oxidase, thereby improving electron transport, generating ATP and influencing ROS signaling2.
However, while these effects appear to be significant, it should be emphasized that their effectiveness heavily relies on the interaction between light and tissue. The latter involves processes such as absorption, scattering and attenuation of optical energy, all of which may be considerably affected by aging. Such changes are mainly connected to the alteration in composition and structure of biological tissues, which include, among other things, the formation of cross-links in collagen fibers, lower content of water and differences in chromophores’ distribution3.
An important feature of PBM is its biphasic dose-response pattern wherein lower dosages cause stimulation, whereas higher dosages may induce inhibition. Such non-linearity underscores the need for proper dosimetry, especially when applying PBM on geriatric patients since tissue sensitivity and optics have changed. Nevertheless, there is a lack of standardization in PBM techniques today and the ideal dosing protocol remains underdeveloped4.
In such cases, computational methods, especially those based on Monte Carlo simulation for photon transport, have proven to be vital tools that help better understand light propagation, fluence and energy deposition processes in biological tissue. In this regard, computer models will provide a way to predict accurately the dose distribution in target tissue layers and allow for optimization of PBM parameters for elderly patients.
Although several quantitative dosimetry schemes have been developed for PBM, no scheme that is specific to the optical properties of aged tissue and fluence attenuation has yet been established.
For this reason, this review attempts to give an integrated look at photo biomodulation processes in aged tissue in terms of biological mechanism, optics and dosimetry optimization and clinical applications. Special attention will be paid to fluence attenuation and biphasic dose-response effects on therapy efficiency. This way, the connection between biological and biophysical aspects of the problem under consideration will be made in order to facilitate the creation of new PBM protocols for geriatric patients.
2. Principles of Photo Biomodulation
Photo biomodulation (PBM), also called low-level laser therapy (LLLT), is a noninvasive treatment approach that employs light from red and near-infrared wavelengths for the modulation of biological responses without thermal effects. PBM does not rely on thermal effects but instead operates through photochemical and photobiological processes unlike high-power laser applications that make use of thermal or ablative effects in achieving biological objectives. The basic processes involved in PBM, including mitochondrial activation, redox processes, regulation of inflammatory responses and tissue repair, are depicted schematically in (Figure 1). The mechanism of action of PBM begins with photon absorption by intracellular chromophores in the tissues leading to series of biochemistry and signaling events. As indicated in (Figure 1), photon absorption causes the activation of mitochondria, increase in ATP formation, controlled ROS formation and activation of transcription factors involved in the control of inflammation and cell proliferation. Thus, the response achieved depends on optical dose and tissue characteristics5.

Figure 1: Mechanisms of photobiomodulation (PBM) at the cellular and molecular level. Diagrammatic representation of the basic mechanisms of PBM. Photobiomodulation involves absorption of red and near infrared light (600 - 980 nm) by mitochondrial chromophores such as cytochrome c oxidase (CCO), which leads to an increase in electron transport activity and increased levels of ATP formation. ROS formation that occurs in a controlled manner acts as signaling molecules responsible for the activation of transcription factors including NF-kB and AP-1, thereby regulating gene expression. As a result, down-regulation of pro-inflammatory cytokines like TNF-α and IL-1β, increased expression of anti-inflammatory cytokines such as IL-10, angiogenesis through VEGF up-regulation and stimulation of collagen synthesis take place.
2.1. Light-tissue interactions
The physics of light-tissue interaction is described by processes such as absorption, scattering, reflection and transmission. As soon as light reaches a biological sample, part of it gets absorbed due to the presence of various chromophores including melanin, hemoglobin and water, whereas the rest is subjected to scattering from tissue inhomogeneity.
As far as photobiomodulation (PBM) applications are concerned, the wavelength region from 600 to 1000 nm or an optical window, is preferable because of low levels of absorption and scattering of photons. Nevertheless, the behavior of light in tissues depends strongly on the characteristics of the latter and age-related changes may affect it dramatically6.
2.2. Mitochondrial photoreception
It has been widely reported that mitochondria act as the chief cellular target in PBM therapy. Cytochrome c oxidase (CCO), a crucial component in the mitochondria’s electron transfer chain, serves as a prime candidate for photoacceptor. The absorption of photon results in electron transfer, mitochondrial membrane depolarization and eventually ATP production.
Furthermore, PBM therapy contributes to the photodissociation of NO from CCO, thus ensuring better oxygen metabolism. While the involvement of CCO is well- documented, several other processes have been suggested as being responsible for photobiomodulation including photon interaction with water bound within mitochondria or other photosensitizers. As depicted in Figure 1 below, these processes suggest that PBM works via a multi-level mechanism rather than a single one7,8.
2.3. Cellular and molecular responses
The primary photochemical effects triggered by PBM cause a chain reaction of other secondary cellular effects, such as increased ATP production, ROS modulation and activation of transcription factors, like NF-κB and AP-
1. In regulated amounts, ROS function as signalers, responsible for the control of gene expression, cell proliferation and adaptation to stressors9.
Photo biomodulation is also effective in reducing inflammatory cytokines (for instance, TNF-α and IL-1β) and stimulating anti-inflammatory cytokine production (for example, IL-10). Additionally, PBM stimulates angiogenesis through VEGF pathways and increases the activity of fibroblasts, causing an increase in collagen formation and extracellular matrix remodeling. The interrelated processes are illustrated in (Table 1) and synthesized in (Figure 1).
Table 1: Cellular and molecular mechanisms of photobiomodulation (PBM) and their biological importance.
|
Mechanism |
Primary Target |
Molecular/Cellular Effect |
Biological
Outcome |
Relevance in Aging Tissues |
References |
|
Photon
absorption |
C y t o c h r o m e coxidase (CCO) |
Activation of electron transport chain |
Initiation of PBM response |
Reduced
efficiency in aged mitochondria → requires optimized dosing |
8,10 |
|
ATP production ↑ |
Mitochondria |
Increased oxidative phosphorylation |
Enhanced cellular energy metabolism |
Restores impaired bioenergetics in aged
cells |
11,12 |
|
ROS
modulation |
Mitochondria / cytoplasm |
Transient increase in
signaling ROS |
Activation of redox- sensitive pathways |
Helps rebalance oxidative stress in aging |
13 |
|
Gene activation |
NF-κB, AP-1 |
Upregulation of transcription and
protein synthesis |
Cell survival and proliferation |
Supports regeneration in aged tissues |
14 |
|
Anti- inflammatory response |
Cytokines (TNF-α, IL-1β, IL-10) |
↓ Pro-inflammatory,
↑ anti- in- flammatory mediators |
Reduced inflammation |
Counteracts “inflammaging” |
12 |
|
Angiogenesis |
VEGF, endothelial cells |
Increased vascular signaling |
New blood
vessel formation |
Improves oxygenation in aged tissues |
15,16 |
|
Collagen synthesis |
Fibroblasts |
Increased extracellular matrix
production |
Tissue remodeling and repair |
Enhances skin and wound
healing in elderly |
17 |
2.4. Biphasic dose response
One of the main features of PBM therapy is the presence of the
biphasic dose-response relation, which is well described by the Arndt-Schulz law. According to the law, small doses
of light activate biological processes, while large
doses may suppress the physiological functions of cells. Thus, the nonlinear
dependency reflects the presence of a special window of therapeutic
action when phototherapy shows
its positive effect.
At lower energies, no effects may be observed
since there is no adequate response from the biological system, while at high energies, cell activation
is suppressed.
Biphasic behavior is especially important
in elderly patients whose metabolism and optical
properties differ significantly from those in young organisms. Thus, strict
regulation of all parameters of irradiation (wavelengths, irradiance, fluence
and time of irradiation) is critical for success in PBM therapy18.
3. Mechanisms of Photo biomodulation in Aging
The mode of action for Photo biomodulation therapy relies on several
mechanisms, which include photochemical reactions, biochemical reactions and
cellular actions. In the context of aging tissue, PBM acts through the
restoration of bioenergetics in cells, regulation of redox signaling, modulation of the immune
response and stimulation of regeneration in tissues. (Table 2) provides an overview of some of the physiological
pathways involved in the action mechanism of photo biomodulation therapy, while
Figure 2 describes how the optical energy distribution affects aging tissues.
3.1. Mitochondrial activation and restoration of cellular bioenergetics
A major pathway in PBM is the uptake of photons at wavelengths
between 600 nm and 1,100 nm into mitochondria by photo acceptors, specifically cytochrome c oxidase. This facilitates enhanced
electron transport and increases mitochondrial membrane potential19.
As aging occurs, mitochondrial metabolism decreases, reducing energy levels and repair rates for tissues.
PBM acts on the mitochondria to help regenerate
cell division and migration as well as metabolic reactions. Also, PBM can
result in the separation of NO from cytochrome c oxidase, thus facilitating
oxidative phosphorylation and oxygen metabolism20.
3.2. Modulation of reactive oxygen species and redox signaling
ROS have a dual impact on biological organisms, as they can act as
destructive substances as well as messengers. PBM induces a controlled increase
in ROS levels that will activate redox-responsive signaling pathways and
transcription factors, including NF-κB and AP-1. Oxidative stress is often high
in older organisms; however, their protective antioxidants may be weakened. PBM works by balancing ROS levels and improving
cell adaptation as well as antioxidant activity in general. It is essential to
maintain control over ROS because this process helps regulate gene expression
and other functions21,22.
3.3. Anti-inflammatory and immunomodulatory effects
One of the features of aging is the chronic low-grade state of inflammation in the body, called
“inflammaging.” PBM downregulates the production of pro-inflammatory molecules,
such
as, TNF-α, IL-1β and cyclooxygenase-2, while upregulating
anti-inflammatory cytokines such as, IL-10.
Moreover, PBM regulates the activity of immune cells, mainly
affecting the process of macrophage polarization and inducing the conversion of
macrophages from M1 phenotypes to M2 phenotypes. This leads to the resolution of inflammation
and remodeling of tissues, which
is extremely important
in cases when the body is aged23,24.
3.4. Stimulation of proliferation, angiogenesis and Tissue regeneration
PBM improves the function of important cell types responsible for tissue repair, such
as fibroblasts, keratinocytes, endothelial cells and stem or progenitor cells. This results in enhanced cell
proliferation, migration and production of extracellular matrix, which in turn
increases tissue regeneration
capacity25,26. Additionally, PBM
induces angiogenesis by increasing the expression of growth factors
like VEGF and TGF-β. Such
actions increase blood flow, oxygen supply and
nutrition delivery, which can be hampered in aging tissues. All of these biological
mechanisms contributing to tissue regeneration are outlined in (Table 2).
Table 2: Mechanistic pathways of photobiomodulation (PBM) and their biological relevance
in aging tissues.
|
Mechanism |
Primary Target |
Key Biological Effects |
Relevance in Aging Tissues |
References |
|
M i t o c h o n d r i a l activation |
Cytochrome c oxidase (CCO) |
Enhanced
electron transport, ↑ ATP production, improved mitochondrial membrane potential |
Restores impaired cellular bioenergetics and
metabolic activity in aged cells |
27 |
|
Nitric oxide photodissociation |
CCO–NO complex |
Release of inhibitory NO, improved oxygen utilization and respiration |
Enhances mitochondrial efficiency under
hypoxic or aged
conditions |
28 |
|
ROS modulation |
Redox-sensitive
signaling pathways |
Transient ROS increase → activation of NF-κB, AP-1,
antioxidant response |
Rebalances
oxidative stress and restores
redox homeostasis |
20,29,30 |
|
Anti-inflammatory regulation |
Cytokines (TNF-α, IL-1β, IL-10) |
↓ Pro-inflammatory mediators, ↑ anti- inflammatory
cytokines |
Reduces chronic inflammation (inflammaging) |
31 |
|
M a c r o p h a g e polarization |
Immune cells
(M1 → M2) |
Shift toward
reparative phenotype, enhanced tissue remodeling |
Promotes resolution of inflammation and healing in elderly tissues |
32 |
|
Cellular proliferation |
Fibroblasts, keratinocytes |
↑ Cell
proliferation, migration, collagen synthesis |
Accelerates delayed wound healing
in aging |
33-35 |
|
Angiogenesis |
VEGF, TGF-β
pathways |
↑ Neovascularization, improved blood supply |
Enhances oxygen
and nutrient delivery to aged tissues |
36-38 |
|
Stem cell
activation |
Mesenchymal stem cells (MSCs) |
↑ Differentiation and regenerative capacity |
Compensates for age-related decline in stem cell
function |
7,39,40 |
|
Optical–tissue interaction |
Tissue chromophores (melanin, Hb,
water) |
Light absorption, scattering, depth- dependent fluence
distribution |
Alters effective dose delivery in aged
tissues |
41-43 |
|
Biphasic dose response |
Cellular metabolic response |
Stimulation at optimal dose, inhibition at excessive dose |
Requires precise
dosimetry in geriatric applications |
18,44-46 |
3.5. Optical and biophysical considerations in aging tissue
Moreover, besides biological factors, the success of PBM therapy is
significantly dependent on the physics of light transport through tissue. With
age, the physical parameters of tissue change due to alterations in collagen structure, hydration, vascularity and chromophore concentration. This
impacts the optical properties of tissues by affecting absorption, scattering
and anisotropy.
(Figure 2(A)) clearly indicates that the intensity of light diminishes from
maximum values at the surface to lower levels at increasing depths. Moreover,
in (Figure 2(B)), it can be observed that fluence is exponentially related
to depth according to the effective attenuation
coefficient (μeff). Consequently, optical changes with age impact the depth of light
penetration into tissue47-49.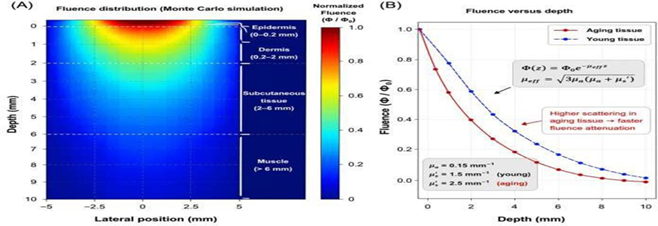
Figure 2: Penetration and fluence
distribution of light
used for photobiomodulation therapy in aging tissues.
Fluence distribution map obtained by Monte Carlo simulation demonstrating light intensity
distribution in a multilayer tissue model, where the absorption is maximal at
the surface layer while the light intensity decreases with depth.
Fluence profile as a function of depth depicting the exponential
decrease in light intensity due to the effective attenuation coefficient (μeff).
3.6. Biphasic dose-response relationship
PBM exhibits a biphasic dose-response relationship response
where small doses cause increased cell activity while large doses can cause
inhibition, with the optimum dose giving the maximum effect. The biphasic
effect of PBM is especially important during use on aged individuals who have
lower metabolic abilities, hence
altering their sensitivity to light. Thus, proper optimization of optical
parameters is necessary for an efficient and
optimized application during treatment of older individuals. Understanding the
physiology of aging and using this information along with optical theory helps
determine the correct treatment procedure50-53.
Despite considerable research into the physiological pathways
involved in photobiomodulation, notable variations can be seen among various
experimental setups. While a large number of researchers have observed improved
mitochondrial function and ATP generation due to exposure to PBM, others have
reported limited or no significant effects based on the wavelength, light intensity and biological conditions of cells54,55.
In addition to the above, the involvement of cytochrome c oxidase as the main photo acceptor
is also disputed, with certain
researchers proposing that it could
involve other molecules such as the water bound to the mitochondria or other
chromophores. The differences suggest that PBM physiology varies among
different tissues and ages.
Hence, there is a need for an extended mechanism that will factor in
the aforementioned differences in order to achieve accurate predictions of PBM
results in aging tissues.
4. Optical Interaction with Aging Tissue
The therapeutic effectiveness of PBM is regulated by both cellular
responses as well as light propagation inside biological tissues. Optical
changes related to aging can have a significant impact on the way in which
light propagates inside biological tissues,
thus impacting the amount of light that can be effectively
delivered, as seen in Figure 2 below. Parameters of light propagation are
highlighted in (Table 3).
4.1. Age-related changes in tissue optical properties
Tissue composition is significantly altered with the process of
aging. These changes in tissue composition directly impact the optical
characteristics. The changes
include decreased water content, changes in the structure of collagen and changes in the concentration of chromophores such as melanin and hemoglobin.
All these changes impact the basic optical parameters such as the absorption coefficient (μₐ), scattering coefficient (μ↑) and the anisotropy factor (g)56.
Changes in the structure of collagen with the process
of aging include increased
collagen cross-linking and disorganization. These changes impact the scattering
characteristics. Similarly, changes in tissue pigmentation and vascularization impact
the absorption characteristics57,58. The changes
in tissue composition with the process of aging
increase the optical heterogeneity of the tissue, which impacts the propagation
of photons.
4.2. Light attenuation and fluence distribution
The propagation of light in biological tissues is affected by
absorption and scattering phenomena. Consequently, there is exponential
attenuation as light travels deeper into tissues. This can be characterized as follows:
?(?) = ? ?−????? … . (?)
Where I (z) represent light intensity at a depth z, I0 represents incident light intensity and μeff represents effective attenuation coefficient. The effective attenuation coefficient can be characterized as follows:
? = √?? (? + ? ′) … . (?)
Where μs′ = μs (1-g) is the reduced scattering coefficient.
As seen from Figure 2(B), fluence falls off sharply with depth, suggesting that a substantial fraction of optical energy is lost to absorption and scattering in the outer layers of tissue. In aged tissues, the enhanced scattering effect causes even greater attenuation of the beam.
4.2. Monte carlo modeling of photon transport
accurate description of the phenomenon. Therefore, the Monte Carlo (MC) simulation has been recognized as the gold standard in the simulation of photon transport59,60.
This approach considers the simulation of the path of single photons as they experience multiple scattering and absorption. The spatial distribution of the MC simulation is presented in Figure 2(A), where the distribution of the photon fluence decreases from the surface with depth. Moreover, the MC simulation offers the possibility of simulating the realistic multi-layer model of the tissue involved. This makes the MC simulation highly appropriate for the simulation of the aging tissues involved.
4.3. Implications for PBM dosimetry in aging
The optical properties of aging tissues have significant implications for PBM dosimetry. As illustrated in Figure 2(A-B), the energy deposition becomes superficial, while the fluence at the deeper layer is greatly reduced. Hence, it is crucial for PBM protocols in geriatric medicine to consider these changes in optical properties by appropriately modifying the parameters used in PBM, including the wavelengths, power density and exposure time52,61. The optical parameters relevant for light propagation and their implications in aging tissues are listed in (Table 3).
4.4. Optimization strategies
Optimization methods for dealing with the problem of light attenuation in aging tissues include:
• Utilization of long wavelength light (800-980 nm) for increased penetration
• Modification of surface fluence to account for attenuation loss at increasing depths
• Utilization of Monte Carlo based simulation models for treatment planning
•Tailored PBM therapy according to tissue or patient specificity
All of these optimization techniques lead to greater light control and PBM efficacy.
Table 3: Optical parameters and their impact on photo biomodulation in aging tissues.
|
Parameter |
Description |
Effect in Aging Tissues |
Impact on PBM |
References |
|
(µa) (absorption coefficient) |
Light absorption by chromophores (melanin, hemoglobin, water) |
Altered chromophore distribution
with age |
Modifies energy deposition profile |
43,62,63 |
|
(µs) (scattering coefficient) |
Photon scattering within tissue microstructure |
Increased due
to collagen cross-
linking and structural changes |
Reduces penetration depth |
62,64,65 |
|
(g) (anisotropy factor) |
Directionality of scattering |
Slight variation with tissue aging |
Influences photon propagation direction |
62,66,67 |
|
(µeff) (effective attenuation coefficient) |
Combined absorption and scattering effects |
Increased in aging tissues |
Accelerates light attenuation |
67,68 |
|
(Φ)
Fluence |
Optical energy
per unit area within tissue |
Reduced at deeper layers |
Limits therapeutic effectiveness in deeper tissues |
68,69 |
5. Clinical Applications of Photobiomodulation in Geriatrics
Photobiomodulation (PBM) has become a highly prospective non-invasive method of treating various aging- related pathologies. Due to its capacity to affect mitochondrial functioning, oxidative stress and inflammation, photobiomodulation becomes an effective way to influence the most important pathological mechanisms of tissue dysfunction related to aging. The connection between biological effects caused by photo biomodulation and clinical results can be seen in (Figure 3); whereas clinical uses of PBM are described in (Table 4).
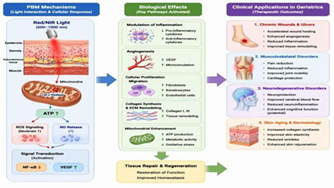
Figure 3: Photobiomodulation (PBM) applications in geriatrics
medicine. Scheme illustrating the connections between the biological
processes initiated via PBM and its therapeutic effects.
Light activation of mitochondrial chromophores increases the
production of ATP and ROS signaling, which results in regulation of
inflammatory responses, neovascularization and tissue regeneration.
5.1. Chronic wounds and ulcers
Chronic wounds like diabetic foot ulcers and pressure ulcers are common among geriatric patients
because of poor vascularization,
chronic inflammation and inability for regeneration. PBM promotes wound healing
through cellular proliferation, inflammation reduction and angiogenesis by
elevating levels of VEGF [70–72].
PBM has also been shown to improve wound healing by
increasing the expression of vascular endothelial growth factor (VEGF), thus
improving wound microcirculation. PBM has also been shown to improve wound
healing by improving the inflammatory response, thus improving the transition
from the inflammatory phase to the proliferative phase of wound healing73.
5.2. Musculoskeletal disorders
Musculoskeletal disorders, including osteoarthritis and joint pain, are significant sources
of disability in the elderly.
PBM has therapeutic effects
in treating musculoskeletal disorders by its anti-inflammatory and analgesic properties, which are achieved by its antioxidant properties in
reducing oxidative stress and inflammatory mediators23,74.
PBM also has effects in improving microcirculation and tissue oxygenation, as well as its effects in improving chondrocyte
function and maintenance of the cartilaginous matrix. This makes PBM an effective adjunctive therapy
in the management of geriatric musculoskeletal disorders21,75.
5.3. Neurodegenerative disorders
Neurodegenerative diseases such as Alzheimer’s
and Parkinson’s disease
have a significant association
with mitochondrial dysfunction, oxidative stress and neurodegeneration. PBM
therapy, especially transcranial PBM therapy, has shown promise as a
neuroprotective therapy for neurodegenerative diseases76.
PBM therapy increases
mitochondrial activity in neurons,
increases blood flow to the brain and decreases neuroinflammation. These mechanisms have shown promise in improving cognitive functions
and neurological outcomes. However, more clinical studies are necessary to
prove the long-term effects and
treatment protocols for PBM therapy for neurodegenerative diseases.
5.4. Skin aging and dermatological applications
Skin aging is characterized by reduced collagen synthesis, decreased
elasticity and degradation of skin structures. PBM has been used for
therapeutic purposes in dermatology for rejuvenation and repair of tissues.
The therapeutic effects
are mediated by enhanced
fibroblast proliferation and collagen synthesis due to increased mitochondrial activity and growth factor secretion.
PBM therapy increases microcirculation and reduces oxidative stress for
improved skin texture, elasticity and dermal structures. Clinical
studies have shown
significant improvement in reducing wrinkles and improving skin quality
after PBM therapy.
5.5. Integration of clinical evidence
Even though photo biomodulation proves to be widely applicable as a
therapy tool in many clinical conditions, inconsistency in therapy
parameters such as wavelength,
fluence, irradiance and exposure
time is an issue. The lack of uniformity
in dosimetric parameters makes comparing different clinical trials rather
challenging.
As can be seen from (Figure
3), the effectiveness of the therapy is directly
related to certain
biological mechanisms associated with activation, regulation of mitochondrial activity and changes
in redox balance
and inflammation. ( Table 4) summarizes the main
applications of PBM in geriatric medicine, the mechanisms that work behind each
application and therapeutic effects observed.
Table 4: Clinical applications of photo biomodulation in geriatric patients.
|
Application |
Mechanism of Action |
Key Biological Targets |
Clinical Outcomes |
References |
|
Chronic wounds
and ulcers |
↑ ATP production, ↑ VEGF, ↓ inflammation |
Fibroblasts, endothelial cells, cytokines |
Accelerated wound healing, enhanced angiogenesis,
improved tissue remodeling |
74,77 |
|
Musculoskeletal disorders |
↓ oxidative stress, ↓ inflammatory mediators, ↑
microcirculation |
Chondrocytes, synovial cells |
Pain reduction, improved joint mobility, enhanced functional recovery |
78 |
|
Neurodegenerative disorders |
↑ mitochondrial function, ↑
cerebral blood flow, ↓
neuroinflammation |
Neurons, microglia |
Improved cognitive performance, neuroprotection,
enhanced neuronal survival |
79 |
|
Skin aging and dermatology |
↑ fibroblast proliferation, ↑ collagen synthesis, ↑ growth factor signaling |
Dermal fibroblasts, extracellular matrix |
Improved skin elasticity, wrinkle
reduction, dermal regeneration |
80 |
Although PBM has shown positive results in clinical settings, its
effectiveness varies among different studies. Factors such as wavelength,
fluence, irradiance and exposure time are different across studies, making it
hard to compare the results. Some
studies show that similar parameters used in PBM therapy may produce varied
results, proving that there is no clear
guideline in the use of PBM
therapy.
Furthermore, clinical studies may be flawed due to factors such as a
small number of participants, inadequate control groups and insufficient follow-ups, leading to unreliable results. The heterogeneous characteristics of the population also make it difficult to interpret the results.
Therefore, the current studies should be improved by conducting
extensive clinical studies and developing a uniform dosimetric guideline for
PBM therapy.
6. Dosimetry and Therapeutic Parameters
Photo biomodulation (PBM) therapy is greatly influenced by dosimetry
accuracy. Parameters such as the wavelength, irradiance, fluence, duration of exposure and frequency should be precisely manipulated in order to attain favorable physiological effects. This becomes
especially significant in aged tissue owing
to the presence of changes in optical properties and metabolism that affect both the
penetration and biological activity of light.
One unique characteristic of photo biomodulation therapy is its dose-dependency, which can be
observed through the nonlinear interaction of light energy on biological processes. The dose-response relationship is depicted in (Figure 4), whereas
the dosimetric parameters involved
in photo biomodulation therapy and their importance in medical practice are detailed
in (Table 5).
6.1. Wavelengths
The wavelength chosen determines how deep the light can penetrate
into the tissue as well as the extent of the absorbance by the chromophores. Red light (630 - 660 nm) and near infrared (800 - 980 nm) are normally used
in PBM treatments43. Red
wavelengths of light have high absorbance and therefore are used for
dermatology purposes and wound treatment; on the other hand, near infrared
light has deeper
penetration and hence is best used to treat internal
tissues such as muscles and joints.
6.2. Power density (Irradiance)
Irradiance, which is measured in mW/cm², describes how quickly
energy can be administered to the tissue. This factor becomes important because very low irradiance would
not have any effect on the cells, while high irradiance
can cause inhibition.
The importance of the irradiance level should be taken into account
together with the duration of exposure, because it will define the amount of energy. In that regard,
it becomes important to optimize the irradiance level
in order to remain within the therapeutic range.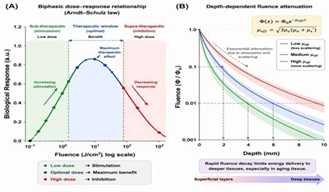
Figure 4: Biphasic nature of the dose response and depth- dependent fluence attenuation for photo biomodulation.
A biphasic nature of the dose-response relationship with demonstration of the
Arndt-Schulz law and optimal therapeutic window.
Depth-dependent fluence attenuation with exponential decrease of
intensity as a result of light absorption and scattering.
6.3. Fluence (Energy density)
Fluence or the amount of energy per unit area (J/cm²) is another very important factor in PBM therapy and is calculated as follows:
??????? = ????? ??????? × ????
????… . (?)
Typical values for fluence are in the 1-10 J/cm² range for
superficial treatments and in the 50–100 J/cm² range for deep tissues.
Nevertheless, due to the absorption and scattering process, surface fluence
does not indicate energy delivery into deeper tissue levels.
6.4. Exposure time
6.5. Dose response and therapeutic window for PBM
It is necessary to determine the proper therapeutic window for each application of PBM, especially in older tissues with different cellular sensitivities and optical properties.
Table 5: Important photo biomodulation dosimetry parameters and ranges.
|
Parameter |
Definition |
Typical Range |
Clinical Relevance |
References |
|
Wavelength (nm) |
Light spectral range used for PBM |
630–660 (superficial), 800–980 (deep) |
Determines penetration depth and chromophore absorption |
81 |
|
Power density
(mW/cm²) |
Power delivered per unit area |
5–500
mW/cm² |
Controls rate of energy
delivery and cellular
stimulation |
44 |
|
Fluence (J/cm²) |
Energy delivered per unit area |
1–10 (superficial),
10–100 (deep) |
Determines therapeutic dose
and effectiveness |
82 |
|
Exposure time (s–min) |
Duration of irradiation |
Seconds to minutes |
Influences total delivered energy |
33 |
|
Treatment frequency |
Number of
sessions |
2–5
sessions/week |
Determines cumulative therapeutic response |
83 |
6.6. Optimal dosage and modeling approach
With the complications associated with light transport through biological tissues in aging, it is essential to use simulation techniques for optimizing the dosimetry procedure. By means of simulations based on the Monte Carlo technique, fluence distribution and energy deposition in layered tissues can be accurately predicted.
It makes it possible to develop a mathematical model describing the relationship between irradiation parameters at the surface and dose delivery in tissues. It can be used to develop individual photobiomodulation programs.
7. Challenges and Limitations of Photo Biomodulation in Geriatrics
Although there is increasing interest in PBM as a potential treatment for age-related diseases, several obstacles exist that inhibit its broad application and reproducibility in clinical practice, especially among older adults.
7.1. Inconsistency of protocols
A major challenge associated with photo biomodulation (PBM) therapy includes the inconsistency of treatment protocols. There is considerable variation in important parameters such as wavelength, power density, fluence and time duration of treatments in various research papers and studies33. In addition, the biphasic nature of PBM’s dose response effect implies that underdosing or overdosing can be detrimental to the treatment process. Establishing reliable protocols, therefore, is essential in order to ensure effective PBM treatment.
7.2. Variations in light penetration depth
However, penetration depth affects the effectiveness of PBM and its optical characteristics determine the ability of light to penetrate tissues. In Section 4 and (Figure 2) below, it was shown that the intensity of light penetrates tissues with exponential decay because of absorption and scattering.
For instance, in older tissues, the amount of light that reaches muscle, joint and neural tissues reduces greatly because of greater scattering and heterogeneous nature of the tissues.
7.3. Patient-specific biological response
Individual biological reactions to PBM also differ greatly depending on the age of the person, their skin color, tissue type, vascular structure, metabolism and health status. When applied to elderly patients, additional variables such as decreased mitochondria performance, poor microcirculation and abnormal immunity affect the results. The unique nature of individual biological reactions to PBM poses challenges for creating standardized PBM treatment regimens.
7.4. Limitations in clinical evidence
While there have been multiple studies documenting positive effects of PBM, the quality and reliability of clinical evidence are highly inconsistent. Different studies have different designs, sample sizes, treatment protocols and evaluation criteria. This makes it difficult to draw conclusions from clinical findings.
Moreover, there are no large-scale randomized control trials that specifically deal with geriatric patients. This makes it impossible to develop guidelines for the use of PBM therapy in geriatrics.
7.5. Limitations of dosimetric and modeling strategies
Although dosimetric modeling techniques like Monte Carlo calculations offer much information about the interaction of light and energy in biological tissue, they too carry certain limitations. This is due to the fact that some models use simplistic assumptions regarding the shape of biological tissue and the optical parameters used in calculations.
The limitation becomes more pronounced in the case of aged tissues, which have greater structural heterogeneity than healthy tissue. In addition, the adoption of modeling methods for clinical applications is still limited.
7.6. Need for personalized and adaptive PBM treatments
Taking into account the interaction of all those factors, such as optical variability, biological differences and dependency on doses, the trend towards personalized therapy is increasingly required. Adaptive methods of PBM treatments based on patient- specific data may help to achieve a higher accuracy of treatment.
The development of PBM protocols using computational simulations, imaging and biosensors is an interesting area that may lead to the design of individually optimized PBM therapy regimens.
Although photo biomodulation shows significant therapeutic potential, several fundamental challenges limit its clinical translation, particularly in aging populations. One of the primary issues is the lack of standardized dosimetric parameters, as variations in wavelength, power density and exposure time can lead to inconsistent biological responses due to the biphasic dose-response effect.
Another critical limitation lies in the uncertainty of light penetration depth in aged tissues. Increased scattering and altered optical properties reduce the amount of energy reaching deeper tissue layers, making it difficult to ensure adequate dose delivery at the target site.
Moreover, current computational models, including Monte Carlo simulations, often rely on simplified assumptions regarding tissue homogeneity and optical properties. These assumptions may not accurately represent the structural complexity and heterogeneity of aging tissues, leading to discrepancies between simulated and real biological outcomes.
In addition, patient-specific variability, including differences in skin pigmentation, vascularization and metabolic activity, significantly affects PBM response. This variability highlights the limitation of generalized treatment protocols and underscores the need for personalized PBM approaches.
Therefore, future research should focus on integrating advanced multiphysics modeling, real-time feedback systems and patient-specific data to improve the accuracy, reproducibility and clinical applicability of PBM therapy.
8. Conclusion and Future Perspectives
Photo biomodulation therapy (PBM) is becoming increasingly popular as an innovative noninvasive technology designed to treat the negative changes associated with aging at the cellular level, affecting such processes as mitochondrial function, oxidation and inflammation response.
The present review reveals the importance of the interplay between photo biomodulation mechanisms, interactions between light and tissue structures and accurate calculation of energy doses in achieving effective treatment of tissue dysfunctions associated with aging. Aging is characterized by numerous physiological changes in tissues, leading to their decreased permeability to light. As a consequence, traditional protocols based on photo biomodulation mechanisms used for healthy tissues cannot be effectively used for elderly patients.
One of the fundamental aspects of PBM technology is the presence of a dose-response curve showing the existence of an optimum range where the treatment effect is observed. Insufficient energy levels cannot produce any biological effect, while overexposure can have a destructive nature.
Innovative computational methods, especially those involving photon transport modeling with Monte Carlo calculations, are valuable means of analyzing light propagation and energy transfer through complicated and heterogeneous biological materials. Thus, incorporating such computational techniques with experimental or clinical data will play an important role in increasing the effectiveness and reproducibility of PBM therapy.
Although PBM shows a great potential to improve health care, there are still some problems related to the absence of uniform protocols, the heterogeneity of clinical data and the biological specificity of aging tissues that have to be solved. To achieve this goal, it is necessary to create scientifically proven guidelines and personalized treatment options based on the optical properties of biological tissue.
Further research must involve the use of Multiphysics modeling, as well as dosimetry and sensor feedback control in order to provide personalized PBM therapy. Besides, it is necessary to conduct large-scale controlled clinical trials to validate treatment protocols and ensure their efficacy.
In summary, the effective implementation of PBM into mainstream medical practice for elderly patients will require an interdisciplinary effort that involves biology, optics and mathematical modeling. Through the integration of these disciplines, PBM can evolve from an empirical form of therapy to one that is precisely engineered for each individual patient.
9. Declarations
9.1. Funding
This work received no particular financial support from the funding bodies in the government, private or non-profit organizations.
9.2. Conflict of interest
The author declares that there is no conflict of interest
9.3. Ethics approval
9.4. Consent to participate
9.5. Data availability
9.6. Author’s contributions
9.7. Consent for publication
9.8. AI tools involved
10. References
1. Zahouani H, Pailler-Mattei C, Sohm B, et al. Characterization of the mechanical properties of a dermal equivalent compared with human skin in vivo by indentation and static friction tests. Skin Research and Technology, 2009;15(1): 68-76.
2. Airan LE, Hruza G. Current lasers in skin resurfacing. Facial Plastic Surgery Clinics of North America, 2005;13(1): 127-139.
3. Kim YJ, Suh HY, Choi ME, et al. Clinical improvement of photoaging- associated facial hyperpigmentation in Korean skin with a picosecond 1064-nm neodymium-doped yttrium aluminum garnet laser. Lasers in Medical Science, 2020;35(7): 1599-1606.
4. Seirafianpour F, Pour Mohammad A, Moradi Y, et al. Systematic review and meta-analysis of randomized clinical trials comparing efficacy, safety and satisfaction between ablative and non-ablative lasers in facial and hand rejuvenation/resurfacing. Lasers in Medical Science. Springer Science and Business Media Deutschland GmbH, 2022.
5. Sommer AP. Mitochondrial cytochrome c oxidase is not the primary acceptor for near infrared light-it is mitochondrial bound water: the principles of low-level light therapy. Annals of Translational Medicine, 2019;7(1): 13.
6. Hamblin MR, Demidova TN. Mechanisms of low-level light therapy. In Mechanisms for Low-Light Therapy. SPIE, 2006;6140: 614001.
7. De Freitas LF, Hamblin MR. Proposed Mechanisms of Photobiomodulation or Low-Level Light Therapy. IEEE Journal of Selected Topics in Quantum Electronics, 2016;22(3): 348-364.
8. Hamblin MR. Mechanisms and Mitochondrial Redox Signaling in Photobiomodulation. Photochemistry and Photobiology. Blackwell Publishing Inc, 2018.
9. Rai V. Chapter 9 Role of Reactive Oxygen Species in Low-Level Laser Therapy. In Handbook of Low-Level Laser Therapy. Jenny Stanford Publishing, 2016: 141-164.
10. Karu TI. Cellular mechanisms of low-power laser therapy. In Laser Applications in Medicine, Biology and Environmental Science. SPIE, 2003;5149: 60.
11. Amaroli A, Benedicenti A, Ferrando S, et al. Photobiomodulation by Infrared Diode Laser: Effects on Intracellular Calcium Concentration and Nitric Oxide Production of Paramecium. Photochemistry and Photobiology, 2016;92(6): 854-862.
12. Karu TI, Pyatibrat LV, Afanasyeva NI. Cellular effects of low power laser therapy can be mediated by nitric oxide. Lasers in Surgery and Medicine, 2005;36(4): 307-314.
13. Gao X, Xing D. Molecular mechanisms of cell proliferation induced by low power laser irradiation. Journal of Biomedical Science, 2009;16(1): 4.
14. Heo JC, Park JA, Kim DK, et al. Photo biomodulation (660 nm) therapy reduces oxidative stress and induces BDNF expression in the hippocampus. Scientific Reports, 2019;9(1): 1-8.
15. de Sousa APC, Paraguassú GM, Silveira NTT, et al. Laser and LED phototherapies on angiogenesis. Lasers in Medical Science, 2013;28(3): 981-987.
16. Al Timimi Z, Najeeb HN, Jasim KM. Investigate the impact of laser dosages on the regeneration of peripheral blood leukocytes after gamma radiation exposure. Radiation Physics and Chemistry, 2024;224: 112056.
17. Wilgus TA. Inflammation as an orchestrator of cutaneous scar formation: a review of the literature. Plastic and Aesthetic Research, 2020;7: 54.
18. Hamblin MR. Shining light on the head: Photo biomodulation for brain disorders. BBA Clinical. Elsevier BV, 2016.
19. Timimi Z. The impact of 980nm diode laser irradiation on the proliferation of mesenchymal stem cells derived from the umbilical cord’s. Tissue and Cell, 2024;91: 102568.
20. Hamblin MR. Mechanisms and applications of the anti-inflammatory effects of photobiomodulation. AIMS Biophysics. American Institute of Mathematical Sciences, 2017.
21. Timimi ZAL, Gide B, Tamimi ZJM. Photobiomodulation therapy in musculoskeletal rehabilitation, mechanisms, clinical evidence and integrated protocols: a systematic review. Sport Sciences for Health, 2026;22(2): 115.
22. De Marchi T, Ferlito JV, Ferlito MV, et al. Can Photobiomodulation Therapy (PBMT) Minimize Exercise-Induced Oxidative Stress? A Systematic Review and Meta- Analysis. Antioxidants. MDPI, 2022.
23. Hussein BR, Al Timimi Z. An Ex-Vivo Study of Photobiomodulation Effects on Hematological and Inflammatory Markers in Breast Cancer Patients. Asian Pacific Journal of Cancer Care, 2026;11(2): 235-242.
24. Shamloo S, Defensor E, Ciari P, et al. The anti-inflammatory effects of photobiomodulation are mediated by cytokines: Evidence from a mouse model of inflammation. Frontiers in Neuroscience, 2023;17: 1150156.
25. de Freitas NR, Guerrini LB, Esper LA, et al. Evaluation of photobiomodulation therapy associated with guided bone regeneration in critical size defects. In vivo study. Journal of Applied Oral Science, 2018;26: 20170244.
26. Chen HY, Tsai HH, Tam KW, et al. Effects of photobiomodualtion therapy on breast cancer-related lymphoedema: A systematic review and meta-analysis of randomised controlled trials. Complementary Therapies in Medicine. Churchill Livingstone, 2019.
27. Tuchin VV. Tissue Optics and Photonics: Light-Tissue Interaction. Journal of Biomedical Photonics & Engineering, 2015;1(1): 98-134.
28. Yan XL, Wu X, Zhou JF, et al. Growth of laser single-crystals Er: YVO4 by floating zone method. Journal of Crystal Growth, 2000;220(4): 543-547.
29. Lunova M, Smolková B, Uzhytchak M, et al. Light-induced modulation of the mitochondrial respiratory chain activity: possibilities and limitations. Cellular and Molecular Life Sciences, 2020;77(14): 2815- 2838.
30. Schäfer M, Werner S. Oxidative stress in normal and impaired wound repair. Pharmacological Research. Academic Press, 2008.
31. Walski T, Dąbrowska K, Drohomirecka A, et al. The effect of red-to-near-infrared (R/NIR) irradiation on inflammatory processes. International Journal of Radiation Biology. Taylor & Francis, 2019.
32. Chen C, Liu T, Tang Y, et al. Epigenetic regulation of macrophage polarization in wound healing. Burns and Trauma. Oxford Academic, 2023.
33. Kreisler M, Christoffers AB, Al-Haj H, et al. Low level 809-nm diode laser-induced in vitro stimulation of the proliferation of human gingival fibroblasts. Lasers in Surgery and Medicine, 2002;30(5): 365-369.
34. Ayuk SM, Houreld NN, Abrahamse H. Effect of 660 nm visible red light on cell proliferation and viability in diabetic models in vitro under stressed conditions. Lasers in Medical Science, 2018;33(5): 1085-1093.
35. Khadra M, Lyngstadaas SP, Haanæs HR, et al. Effect of laser therapy on attachment, proliferation and differentiation of human osteoblast- like cells cultured on titanium implant material. Biomaterials, 2005;26(17): 3503-3509.
36. Stepanov YV, Golovynska I, Golovynskyi S, et al. Red and near infrared light-stimulated angiogenesis mediated via Ca2+ influx, VEGF production and NO synthesis in endothelial cells in macrophage or malignant environments. Journal of Photochemistry and Photobiology B: Biology, 2022;227: 112388.
37. Chaves ME de A, Piancastelli ACC, de Araújo AR, et al. Effects of low-power light therapy on wound healing: LASER x LED. Anais Brasileiros de Dermatologia. Sociedade Brasileira de Dermatologia, 2014.
38. Bacci S, Bassetto F, Corsi A, et al. Photobiomodulation in clinical practice. Veins and Lymphatics, 2023;12(1): 11821-11906.
39. Khorsandi K, Hosseinzadeh R, Abrahamse H, et al. Biological Responses of Stem Cells to Photobiomodulation Therapy. Current Stem Cell Research & Therapy, 2020;15(5): 400-413.
40. Chailakhyan R, Grosheva A, Vorobieva N, et al. Thermo- photobiomodulation of stem cells. In BIO Web of Conferences. EDP Sciences, 2024;113: 06006.
41. Kulikov K, Koshlan T. Laser interaction with heterogeneous biological tissue: mathematical modeling. Cham: Springer International Publishing, 2018.
42. Niemz MH. Interaction Mechanisms. In Laser-Tissue Interactions. Springer, 2002: 45-149.
43. Farhad H, Mohamad J, Asaad H, et al. Influences of different low level laser power at wavelength 635 nm for two types of skin; dark and light. Proceedings of the 7th IMT-GT UNINET and the 3rd International PSU-UNS Conferences on Bioscience Influences, 2009;7(3): 130-135.
44. Nie F, Hao S, Ji Y, et al. Biphasic dose response in the anti- inflammation experiment of PBM. Lasers in Medical Science. Springer Science and Business Media Deutschland GmbH, 2023.
45. Huang YY, Chen ACH, Carroll JD, et al. Biphasic dose response in low level lightherapy. Dose- Response, 2009;7(4): 358-383.
46. Flores Luna GL, De Andrade ALM, Brassolatti P, et al. Biphasic Dose/Response of Photo biomodulation Therapy on Culture of Human Fibroblasts. Photo biomodulation, Photomedicine and Laser Surgery, 2020;38(7): 413-418.
47. Lamster IB, Asadourian L, Del Carmen T, et al. The aging mouth: differentiating normal aging from disease. Periodontology 2000. John Wiley & Sons, Ltd, 2016.
48. Vaughan MB, Spencer CL, Goddard JD, et al. Effect of near- infrared lasers on myofibroblast differentiation and contraction. In Biophotonics and Immune Responses VII. SPIE, 2012;8224: 8224.
49. Liebert A, Capon W, Pang V, et al. Photophysical Mechanisms of Photo biomodulation Therapy as Precision Medicine. Biomedicines. Multidisciplinary Digital Publishing Institute, 2023.
50. Zein R, Selting W, Benedicenti S. Effect of Low-Level Laser Therapy on Bone Regeneration during Osseointegration and Bone Graft. Photomedicine and Laser Surgery, 2017.
51. Pires Marques EC, Piccolo Lopes F, Nascimento IC, et al. Photobiomodulation and photodynamic therapy for the treatment of oral mucositis in patients with cancer. Photodiagnosis and Photodynamic Therapy, 2020;29: 101621.
52. Al Timimi Z. Simulated dose-dependent effects of 660 nm laser photostimulation on human sperm motility and acrosome integrity using MATLAB modeling. Lasers in Medical Science, 2025;40(1): 418.
53. Razavi P, Jafari A, Vescovi P, et al. Efficacy of Adjunctive Photobiomodulation in the Management of Medication-Related Osteonecrosis of the Jaw: A Systematic Review. Photobiomodulation, photomedicine and laser surgery. Mary Ann Liebert, 2022.
54. Al-Timimi Z. Illuminating the path: the role of photodynamic therapy in comprehensive periodontal treatment. Irish Journal of Medical Science, 2025;1971: 1-14.
55. Timimi Z, Mohsen D. Advancements in Deep Wounds Therapies: The Synergistic Application of Laser Therapy and Nanomaterials. International Journal of Lower Extremity Wounds. SAGE Publications Inc, 2025.
56. Oliveira LMC, Tuchin VV. Tissue Optics. In SpringerBriefs in Physics. Springer, Cham, 2019;995: 1-15.
57. Zahra ATT. A comparative study of determination the spectral characteristics of serum total protein among laser system and spectrophotometric: Advantage and limitation of suggested methods. Current Analytical Chemistry, 2019;15(5): 583-590.
58. Tsume Y, Igawa N, Drelich AJ, et al. The in vivo predictive dissolution for immediate release dosage of donepezil and danazol, BCS class IIc drugs, with the GIS and the USP II with biphasic dissolution apparatus. Journal of Drug Delivery Science and Technology, 2020;56.
59. Torres-García E oros-Pantoja R, Aranda-Lara L, et al. A new Monte Carlo code for light transport in biological tissue. Medical and Biological Engineering and Computing, 2018;56(4): 649-655.
60. Rogers DWO. Fifty years of Monte Carlo simulations for medical physics. Physics in Medicine and Biology. IOP Publishing, 2006.
61. Amaroli A, Pasquale C, Zekiy A, et al. Photobiomodulation and Oxidative Stress: 980 nm Diode Laser Light Regulates Mitochondrial Activity and Reactive Oxygen Species Production. Oxidative Medicine and Cellular Longevity, 2021;2021(1): 6626286.
62. Anderson RR, Parrish JA. The optics of human skin. Journal of Investigative Dermatology, 1981;77(1): 13-19.
63. Laakso L, Richardson C, Cramond T. Factors affecting Low Level Laser Therapy. Australian Journal of Physiotherapy, 1993;39(2): 95-99.
64. Bashkatov AN, Genina EA, Kochubey VI, et al. Optical properties of human skin, subcutaneous and mucous tissues in the wavelength range from 400 to 2000 nm. Journal of Physics D: Applied Physics, 2005;38(15): 2543-2555.
65. Mustafa FHFHFH, Jaafar MSMS, Ismail AHAHAH, et al. Red Diode Laser in the Treatment of Epidermal Diseases in PDT. World Academy of Science, Engineering and Technology, 2010;4(10): 677-680.
66. Genina EA, Bashkatov AN, Sinichkin YP, et al. Optical clearing of biological tissues: prospects of application in medical diagnostics and phototherapy. Journal of Biomedical Photonics & Engineering, 2015;1(1): 22-58.
67. Cheong WF, Prahl SA, Welch AJ. A Review of the Optical Properties of Biological Tissues. IEEE Journal of Quantum Electronics, 1990;26(12): 2166-2185.
68. Fang, Q., & Boas, D. A. (2009). Monte Carlo Simulation of Photon Migration in 3D Turbid Media Accelerated by Graphics Processing Units. Optics Express, 2009;17(22): 20178.
69. Wang L, Jacques SL, Zheng L. MCML-Monte Carlo modeling of light transport in multi-layered tissues. Computer Methods and Programs in Biomedicine, 1995;47(2): 131-146.
70. Khalkhal E, Rezaei-Tavirani M, Zali MR, et al. The evaluation of laser application in surgery: A review article. Journal of Lasers in Medical Sciences, 2019;10(4): 104-111.
71. Al-Timimi Z, Mustafa FH. Recognizing the effectiveness of the diode laser 850nm on stimulate the proliferation and viability of mice mesenchymal stem cells derived from bone marrow and adipose tissue. Iraqi Journal of Veterinary Sciences, 2018;32(2): 285-290.
72. Al Timimi Z, Al-Rubaye AF, Diwan DM. A comprehensive study of laser use in dermatology: assessing the safety, innovations and effectiveness of laser technology for skin treatment. Irish Journal of Medical Science. Springer Science and Business Media Deutschland GmbH, 2025.
73. das Neves LMS, Leite G de PMF, Marcolino AM, et al. Laser photobiomodulation (830 and 660 nm) in mast cells, VEGF, FGF and CD34 of the musculocutaneous flap in rats submitted to nicotine. Lasers in Medical Science, 2015;32(2): 335-341.
74. Al-Timimi Z. Evaluation of the Significance of Constant Laser Therapy, 532 nm, in Various Exposure Times on the Healing Process of Wounds Infected by Acinetobacter baumannii. International Journal of Lower Extremity Wounds, 2022;21(4): 640-646.
75. AL-Timimi Z. Examining the combined benefits of photo biomodulation and apigenin for the treatment of asthenozoospermia: An innovative therapeutic strategy. Photochemical and Photobiological Sciences, 2024;23(10): 1945-1955.
76. Zafari J, Jouni FJ, Nikzad F, et al. Combination of Dental-Capping Agents with Low Level Laser Therapy Promotes Proliferation of Stem Cells from Apical Papilla. Photo biomodulation, photomedicine and laser surgery, 2023;41(1): 3-9.
77. Al Timimi Z. Evaluation of the Detrimental Impact of Low-Intensity Laser Radiation on the Characteristics of Sperm Movement, Motion and DNA Damage. Current Applied Science and Technology, 2025;25(2): 0262524.
78. Al Timimi Z. Photodynamic Targeting of HEp-2 and AMN3 Cancer Cells by Hematoporphyrin Activation with a 635 nm Diode Laser. Biophysical Reviews and Letters, 2025;20(02): 105-115.
79. Tsai SR, Hamblin MR. Biological effects and medical applications of infrared radiation. Journal of Photochemistry and Photobiology B: Biology, 2017.
80. Naskar A, Kim KS. Recent advances in nanomaterial-based wound- healing therapeutics. Pharmaceutics. MDPI AG, 2020.
81. Sklar LR, Burnett CT, Waibel JS, et al. Laser assisted drug delivery: A review of an evolving technology. Lasers in Surgery and Medicine, 2014;46(4): 249-262.
82. Karu TI. Mechanisms of interaction of monochromatic visible light with cells. In Effects of Low-Power Light on Biological Systems. SPIE, 1996;3198: 2-9.
83. Crochet JJ, Gnyawali SC, Chen Y, et al. Temperature distribution in selective laser-tissue interaction. Journal of Biomedical Optics, 2006;11(3): 034031.