Isolated Uvular Angioedema Triggered by Peanut Allergy in A 28-Year-Old Male: A Case Report
Abstract
Background: Isolated uvular
angioedema (Quincke’s disease) is a rare manifestation of food allergy, often
caused by a type I
hypersensitivity reaction. While peanut allergies are common, adult-onset
reactions after long-term avoidance are underreported.
Case Presentation: A 28-year-old
Ethiopian male with a childhood-diagnosed peanut allergy presented with
acute-onset dysphagia, throat heaviness, and voice changes following accidental
peanut ingestion. Physical examination revealed isolated uvular edema without
systemic anaphylaxis or airway compromise. Prompt treatment with epinephrine,
corticosteroids, and antihistamines led to complete resolution within 24 hours.
Conclusion: This case highlights the importance of recognizing isolated uvular angioedema as a potential allergic reaction, even in patients with long-standing avoidance of known allergens. Early intervention with epinephrine and adjunctive therapies can prevent progression to severe anaphylaxis.
Keywords: Angioedema, Uvula, Quincke’s disease,
Epinephrine, Case report
1. Introduction
Isolated uvular angioedema (Quincke’s disease)
represents an uncommon but clinically significant form of localized upper
airway swelling. This condition can develop from various etiologies, including
allergic reactions to foods or environmental triggers, medication side effects
(particularly ACE inhibitors and NSAIDs), hereditary angioedema disorders,
mechanical trauma to the oropharynx, or underlying infections1.
While isolated uvular angioedema has been
documented in several case reports, only three published cases specifically
link it to peanut ingestion. This condition typically results from a type I hypersensitivity
reaction. Importantly, clinicians must distinguish it from infectious uvulitis,
which often occurs with epiglottitis and has a different etiology2.
Angioedema is characterized by non-pitting
swelling that develops in subcutaneous and submucosal tissues due to increased
vascular permeability and plasma extravasation3. This condition
occurs when the immune system abnormally responds to harmless substances,
triggering the production of IgE antibodies. These antibodies bind to mast
cells, which are crucial components of the innate immune response. Upon
allergen exposure, activated mast cells degranulate and release potent
inflammatory mediators, including histamine and leukotrienes. This cascade
leads to localized or systemic manifestations such as tissue swelling,
urticaria, mucosal inflammation, and potentially life-threatening airway compromise
in severe cases. The resulting vascular leakage and smooth muscle contraction
contribute to the characteristic clinical presentation of angioedema3-5.
The primary focus in managing Quincke’s edema
is ensuring proper airway protection. Treatment involves close monitoring,
oxygen supplementation, and medications including epinephrine for severe
reactions, antihistamines (H1 and H2 blockers), and corticosteroids such as
dexamethasone. Most documented cases present as acute episodes treated in emergency
settings, often requiring only short-term medical intervention. The majority of
patients respond well to this approach, with many experiencing single
occurrences without recurrence1,6.
2. Case Presentation
A 28-year-old Ethiopian male presented to the
emergency department with a two-hour history of mild dysphagia, throat
heaviness, and voice changes after accidental peanut ingestion. The patient had
a known peanut allergy diagnosed in early childhood but had avoided peanuts
since age five with no prior exposures or reactions in adulthood. His symptoms
began shortly after consuming a meal that was later found to contain peanuts.
Notably, he did not experience any shortness of breath, urticaria, facial
swelling, or other systemic signs of anaphylaxis.
On examination, the patient was
hemodynamically stable with normal vital signs. Oropharyngeal inspection
revealed a markedly swollen and erythematous uvula without involvement of the
tonsils, palate, or tongue (Figures 1 and 2). Nasolaryngoscopy confirmed isolated uvular edema with no
compromise of the airway or vocal cord abnormalities. Laboratory
investigations, including complete blood count and inflammatory markers, were
unremarkable.
Given his known peanut allergy and acute-onset symptoms, he was treated promptly with intramuscular epinephrine (0.3 mg), intravenous dexamethasone (8 mg), and oral cetirizine (10 mg). His symptoms improved significantly within four hours, and the uvular edema resolved completely by the following day.
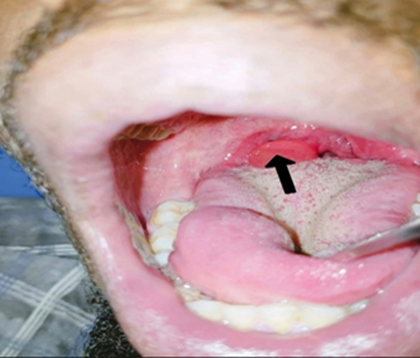
Figure 1: A markedly enlarged, erythematous uvula (black arrow) without involvement of the soft palate or tongue.

Figure 2: Oropharyngeal view indicating a markedly enlarged, erythematous uvula (white arrows) without involvement of the tonsils, palate, or tongue.
3. Discussion
Angioedema is most commonly caused by a type I, anaphylactic,
IgE-mediated or immediate hypersensitivity reaction to a food, drug, insect
venom, preservative, latex product, or aeroallergen7. In recent years, the
incidence of adult-onset food allergies has risen significantly, accounting for
40% to 60% of all allergy cases that develop during adulthood5.
The condition typically manifests as uneven,
mildly painful swelling of the face, lips, and tongue, and can also affect the
hands, feet, or genital area4. In this particular case, a hypersensitivity
reaction to peanuts led to isolated uvular angioedema-a less common but notable
symptom of anaphylaxis. Isolated uvular angioedema, first described by Quincke
in 1882 (also known as Quincke’s disease), is a rare form of upper airway
angioedema. The condition can result from various factors, including hereditary
angioedema, physical trauma, inhalation irritants, food allergies, drug
reactions, and infections. Typically, isolated uvular swelling arises from a
type I hypersensitivity reaction2.
Quincke’s disease refers specifically to
localized non-hereditary angioneurotic edema of the uvula, without any genetic
or laboratory association8. In this case, the patient developed isolated uvular edema
following peanut ingestion with normal laboratory results.
Symptoms can vary between cases, but the most frequently
reported ones include throat discomfort, a sensation of a foreign body,
dysphagia (difficulty swallowing), and throat pain. Some documented cases also
describe hoarseness, choking, snoring, respiratory distress, and even
obstructive sleep apnea1. In this patient, the presenting symptoms were throat
discomfort, a foreign body sensation, and voice changes.
Epinephrine serves as the primary treatment
for anaphylaxis, and delayed administration may lead to severe complications
such as biphasic anaphylaxis or fatal outcomes. During an allergic reaction,
histamine-induced vasodilation and increased vascular permeability contribute
to inflammatory swelling. As secondary interventions, antihistamines and
glucocorticoids are used to help suppress the allergic response and reduce the
effects of histamine release5,6. This case was treated with epinephrine, a
steroid, and an antihistamine.
4. Conclusion
This case demonstrates that isolated uvular
angioedema can occur as an atypical presentation of peanut allergy, even after
prolonged allergen avoidance. Despite the absence of systemic anaphylaxis,
prompt recognition and treatment with epinephrine, corticosteroids, and
antihistamines were crucial in ensuring a rapid recovery. Clinicians should
maintain a high index of suspicion for allergic uvular edema in patients with
known food allergies, as delayed intervention could lead to airway compromise.
This report reinforces the need for patient education on allergen avoidance and
emergency management, even in cases of long-term remission.
5. Authors’ Contributions
Dr. Mohammedsefa Arusi and Dr. Zelalem Tadesse contributed to data acquisition, interpretation of data, critical revision of the manuscript, and final approval of the version to be published. Both authors reviewed and approved the manuscript.
6. References
- Medicina U. Quincke’s disease: a rare clinical disorder. A case
report. Medicina. 2025;1: 84-89.
- Cevik Y, Vural S, Kavalci C. Isolated uvular angioedema:
Quincke’s disease. Am J Emerg Med. 2010;28(4): 493-4.
- Ibrahim S. A case of trauma-related angioedema of the airway in
a patient on an angiotensin receptor blocker. Clin Case Rep. 2024: 1-4.
- Johny T, Juan T. Angioedema: a case
report and review of the literature. J Clin Emerg Med. 2024;5(1): 1-5.
- Nguyen L, Stead TS, Ortiz CL, et al. Anaphylaxis presenting
as uvulitis. Cureus. 2021;13(9): 17834.
- Bernstein JA, Cremonesi P, Hoffmann TK, et al. Angioedema in
the emergency department: a practical guide to differential diagnosis and
management. Int J Emerg Med. 2017;10(1): 15.
- Leung AKC, Robson WLM. Penile and oral angioedema associated with peanut ingestion. Pediatr Emerg Care. 2006;22(4): 256-258.
- Kattel K. Quincke’s disease: isolated uvular angioedema, a
disease entity of unknown etiology. J Med Case Rep. 2023: 1-4.