Recent Advances in Treating Atopic Dermatitis
Abstract
Atopic dermatitis (AD) is a chronic, recurrent
inflammatory skin condition and the leading cause of the global burden from
skin disease. The etiology of AD is multifactorial, including genetic
predisposition, skin barrier dysfunction, immunological dysregulation caused by
T-helper cell imbalances, environmental factors (allergens, pollutants and
climate) and stress.
Diagnosis of AD is based on clinical criteria, which
are supplemented by allergen testing and, in certain circumstances, skin
biopsies. Treatment of AD is individual
and should be tailored to the respective patient. Beside basic therapy (emollients and avoidance of
allergens), current therapeutic options include topical and systemic
corticosteroids, calcineurin inhibitors, biologics (dupilumab, tralokinumab,
lebrikizumab and recently approved nemolizumab), Janus kinase (JAK)inhibitors (baricitinib,
abrocitinib, upadacitinib), phototherapy and psychosomatic counselling. The current European and US-American guidelines on the management of AD
adhere to a stepwise treatment approach, starting with topical therapies and
extending to systemic therapies in moderate to severe cases. Novel topical therapies such as JAK inhibitors (ruxolitinib,
delgocitinib), phosphodiesterase 4 (PDE4) inhibitors (crisaborole, difamilast,
roflumilast) and the aryl hydrocarbon receptor agonist tapinarof have recently been
approved in the US and Japan.
This review presents the most recent advances in
understanding and treating atopic dermatitis. A special focus is given to recent
developments within the AD drug pipeline. The most advanced new drug
developments are the monoclonal antibody amlitelimab targeting the OX40/OX40L
pathway and the oral TYK2 inhibitor ICP-332 for systemic administration. Novel
topical therapies include ointments of pan-JAK inhibitors MH004, CGB-500 and
LNK01004 and the antimicrobial gel zabalafin.
Keywords: Atopic dermatitis, Biologics, PDE4 inhibitors, JAK
inhibitors, Novel drugs
1. Introduction
Atopic dermatitis (AD) is s a chronic, recurrent inflammatory skin
condition and the leading cause of the global burden from skin disease. Chronic
recurrent eczema, severe itching, dry and sensitive skin, often beginning in
early childhood, as well as a family or personal history of atopy (asthma, hay
fever) are important characteristics of AD. Typical distribution patterns of AD
lesions are depending on age. In infants (i), eczema lesions are often more
acute than in adults and mainly located on the face and the extensor surfaces
of the limbs. The trunk might be affected but the nappy area is typically
spared. From age 1-2 years and onwards (ii), polymorphous manifestations with
different types of skin lesions are seen, particularly in flexural folds. In
adolescents and adults (iii), often lichenified and excoriated plaques are
found, particularly at flexures, wrists, ankles and eyelids; in the
head-and-neck type, the upper trunk, shoulders and scalp are involved. Adults
might have only chronic hand eczema or they might present with prurigo-like
lesions1. Clinical manifestations include acute flare-ups with
erythematous, exudative lesions, chronic phases with lichenification,
hyperkeratosis; often accompanied by agonising itching (pruritus), which can
severely impair sleep and quality of life. Atypical vascular reactions,
keratosis pilaris, ichthyosis and periorbital changes can facilitate diagnosis.
Other chronic dermatological diseases with similar phenotypes such as
psoriasis, seborrheic eczema, contact dermatitis, ichthyosis, scabies,
cutaneous lymphomas need to be excluded to assure correct AD diagnosis.
The prevalence of AD varies significantly between geographic regions,
age and sex groups (more frequent in children and women) and diagnostic
criteria. Epidemiological studies from 1992 to 2022 showed that around 101.27 million adults and
102.78 million children worldwide have AD, corresponding to prevalence rates of
2.0% (95% UI 1.4–2.6) and 4.0% (95% UI 2.8–5.3), respectively2. The prevalence of AD is rising worldwide. A recent survey conducted by a polling company between January
and April 2023, targeted individuals aged 16 years or older in 20 countries
across five continents, demonstrated that AD now affects nearly 10% of
individuals of 16 years and over. The highest prevalence was observed in Asia
(e.g., South Korea 15.3% and China 15.1%) followed by Europe (e.g., Spain
13.1%) and Latin America (e.g., Mexico 10.7%), with North America (e.g., USA
7.3%) and Africa (e.g., 7.2%) showing the lowest rates. AD was significantly
more common in female patients across all regions, a finding that is consistent
with previous studies3.
The etiology of AD is multifactorial, including
genetic predisposition (e.g., filaggrin mutations), skin barrier dysfunction,
immunological overreaction, environmental factors (allergens, pollutants) and
stress. In addition, the Western life-style (increased hygiene standards
including the inadequate use of antimicrobials and a diet poor in fibres and
rich in saturated fats and carbohydrate sweeteners) may reduce the skin and gut
microbiome especially during early childhood and as a consequence reduce the
activation of regulatory dendritic cells and regulatory T cells (Tregs)
resulting in a prevalent stimulation of T helper 2 (TH2) cell responses and allergic
disease such as atopic eczema4. In
addition, nerve fibres in the skin produce neuropeptides, which can activate
immune cells and induce inflammation. The TH2 cytokines IL-4, IL-13 and IL-31
generated by immune cells can activate nerve endings and increase itching,
resulting in a vicious itch-scratch cycle that deteriorates skin integrity5 (Figure 1). More recently, the OX40–OX40
ligand (OX40L) axis has been identified as a costimulatory pathway that
promotes immune responses resulting in persistent skin inflammation in AD.
Under inflammatory conditions, OX40L is upregulated on antigen-presenting cells
(APCs) following antigen presentation, contributing to the activation of
antigen-specific TH2 and TH1/TH17/TH22 cells and secretion of proinflammatory
cytokines6. A recent multi-ancestry genome-wide association
meta-analysis of 56,146 AD cases and 602,280 controls, found 101 genome-wide
significant loci associated with AD, with 15 loci that have not been previously
reported. Using a cell-type enrichment analysis, T cells were identified as the
top enriched cell type in AD7.
Taken together, T-cell-mediated processes are the main drivers of pathogenic
hyperinflammation in AD and, at the same time, the main targets of current AD
therapy.
Figure 1: Pathogenesis of atopic
dermatitis.
AMP = adenosine
monophosphate, IFN = interferon, IL = interleukin, JAK = Janus kinase, MDC =
macrophage-derived chemokine, STAT = signal transducer and activator of
transcription proteins, TARC = thymus and activation-regulated chemokine, TSLP
= thymic stromal lymphopoietin (also known as chemokine CCL17)5.
2. Management of Atopic Dermatitis
Management of AD is individual and should be tailored to the respective
patient. Joint decision-making between doctor and patient is important. Treatment
of AD consists of a basic therapy (emollients to support the skin barrier);
topical therapy (glucocorticoids, calcineurin inhibitors) and in more severe
cases systemic therapy (glucocorticoids, biologics, Janus kinase inhibitors).
Compliance to proactive therapy (long-term use of topical anti-inflammatory
agents on affected skin areas, combined with emollients to prevent recurrence)
and in general a healthy lifestyle is crucial to reduce frequency of flares.
Atopic dermatitis may regress in adulthood, but many patients experience
persistent or recurrent symptoms and AD may worsening due to stress, climatic factors
and infections, often associated with other atopic diseases such as asthma,
allergic rhinitis, food allergies; increased risk of mental disorders and sleep
disorders.
Regular clinical assessments should include a periodical
monitoring of the skin through physical examination to assess the severity and
progress of the eczema. The use of objective scores
is recommended to evaluate lesion extent, severity and quality of life impact. Objective
severity scores, such as the eczema area and severity index (EASI), SCORing
atopic dermatitis (SCORAD), investigator’s global assessment (IGA) and
patient-oriented eczema measure (POEM), enable personalized treatment plans and
enhance research comparability. The EASI score integrates body surface area and
skin lesion intensity into a single composite score. The EASI assesses only
active acute or chronic AD lesions, while the SCORAD also assesses dry skin,
pruritus and insomnia8 (Table 1). In addition, the Peak Pruritus Numerical Rating Scale
(PPNRS) can help to quantify and track itch relief and is frequently used as a
patient-reported outcome in clinical trials. The PPNRS is a well-defined,
reliable, fit for purpose measure to evaluate patient-reported intensity of
worst itch in the previous 24 h for adults with moderate-to-severe atopic
dermatitis. Clinical response is indicated by a ≥ 2–4-point change from
baseline in the PP-NRS score9.
Table 1:
Commonly used severity scores for atopic dermatitis8.
|
Score |
Assessment criteria |
No
eczema |
Slightly
detectable eczema |
Mild |
Moderate |
Severe |
Very
Severe |
|
EASI |
Extent (0–100%), Severity of lesions (0–12) |
- |
- |
0-7 |
8-21 |
22-48 |
49-72 |
|
SCORAD |
Extent (0–100%), Intensity (0–3), Subjective
symptoms (0–4) |
- |
- |
0-24 |
25-49 |
50-74 |
75-103 |
|
IGA |
Overall severity |
0: Clear |
1: Almost clear |
2: light pink, slightly raised |
3: pink, moderately raised |
4: deep pink, greatly raised |
5: fiery red, greatly raised |
|
POEM |
Patient‑reported symptoms (7 items, 0–4), Impact (7
items, 0–4) |
0–2: Clear or almost clear |
3-7 |
8-12 |
13-18 |
19-28 |
|
|
EASI = eczema area and severity index, SCORAD =
SCORing atopic dermatitis, IGA = investigator’s global assessment, POEM =
patient‑oriented eczema measure |
|||||||
3. Treatment of Adults with AD
Basic measures include the
regular use of moisturisers to strengthen the skin barrier, appropriate skin
cleansing (e.g., short baths) and avoidance of triggers. The recent updates of
the European and US-American guidelines on the management of AD adhere to a
stepwise treatment approach, starting with topical therapies and extending to
systemic therapies in moderate to severe cases10,11
(Figure 2). Acute
flare-ups are treated with topical corticosteroids, supplemented with
non-steroidal creams containing calcineurin inhibitors such as tacrolimus or
pimecrolimus if necessary. Antimicrobial therapy can be necessary, especially
for infections with Staphylococcus aureus. Frequent local antimicrobial therapy
should be avoided to prevent antimicrobial resistances; systemic antibiotics
are used only for large-area infections. Systemic
therapy is required if the symptoms cannot be controlled sufficiently with
topical treatments and UV-B small band light therapy. However, phototherapy
must not be used in patients with a history of skin cancer or with an increased
risk of skin cancer (including photodamaged skin and those on systemic
immunosuppressants). Topical steroids must be used with care to avoid skin thinning. Topical
antibiotic, antiviral or antifungal treatments should be administered only for
the treatment of superinfections of the skin, not for the treatment of atopic
dermatitis itself. In severe cases, systemic medications such as conventional
systemic immunosuppressants (CSI), monoclonal antibodies targeting inflammatory
cytokines (biologics) or JAK inhibitors (JAKi) may be considered. The JAK
inhibitors baricitinib, abrocitinib and upadacitinib are fast-acting, whereas
the TH2-responses blocking antibodies dupilumab (targeting IL-4 receptor-alpha subunit, IL-4Rα), tralokinumab and lebrikizumab (both targeting IL-13), as well as the
recently approved nemolizumab (targeting IL-31 receptor-alpha subunit, IL-31Rα)
need some weeks to reach full efficacy. CSI such as cyclosporine and systemic
corticosteroids have a rapid onset of action and can be used to treat flares or
to bridge the time until onset of action of slower acting systemic
immunosuppressants such as methotrexate (MTX) and azathioprine (AZT), both of
them can be used off-label in the clinics. MTX must not be used during
pregnancy in contrast to AZT. Oral corticosteroids should only be used as
rescue medication for a short period of time to avoid side effects.
Figure 2: Stepped-care plan for adults, children and adolescents with atopic
dermatitis.

*Crisaborole ointment,
roflumilast cream, ruxolitinib cream, difamilast ointment, ruxolitinib cream
and tapinarof cream with marketing authorisation for atopic dermatitis in the
USA but not in Europe.
Abbreviations: AhRa = aryl hydrocarbon receptor agonist, CIS = conventional
immunosuppressants, JAKi = JAK inhibitors, PDE4i = PDE4 inhibitors, TCI =
topical calcineurin inhibitors, TCS = topical corticosteroids10-12.
4. Treatment of Children and Adolescents with AD
About 80% of AD
patients are identified in the early childhood and the comorbidity with asthma
is a common allergic condition. A significant proportion of children shows
symptoms before 12 months of age (approximately 60 %) and close to 80% before
the age of 61. While it often
improves or goes away as children get older, it can persist into adulthood or,
less commonly, have its first onset in adult life. Thinking about 50 years ago
parents treated their children with fatty and oily zinc ointments, oak bark
pouches to achieve itch relief or ‘Cramer bandages’ to protect the child’s body
against scratching. Nowadays, more solutions for everyday use are available
such as soft cotton gloves protecting from scratching and several basic care
products (gentle, moisturizing products) to be used after washing immediately
after getting up and again in the evening before going to bed.
Nowadays, treatment
options for children with moderate to severe AD have expanded enormously: the
anti-IL-4Rα antibody dupilumab is available for children older than 6 months,
the two IL-13 antibodies tralokinumab and lebrikizumab and the IL-31Rα antibody nemolizumab are available from the age of 12 years. From the group of JAK
inhibitors, baricitinib is approved (in Europe and more than 30 countries
worldwide except the USA) from the age of 2 and upadacitinib and abrocitinib
from the age of 12 for the treatment of children with moderate to severe AD.
The approval of these systemic therapies represents a major change in the lives
of severely affected children, which has a significant impact on their social
participation and educational success. Overall, the side effect profile of
systemic drugs in children is generally better than in adults, with specific
challenges being the planning of live vaccinations and the administration of
injections. The European Guideline on
Atopic Eczema also recommends a stepwise treatment approach for paediatric AD
patients, starting with topical therapies in mild AD and extending to systemic
therapies for moderate to severe AD, similar to the recommendations for adults,
except that systemic corticosteroids and PUVA-phototherapy should be avoided10. Similarly, the American Academy of Dermatology has recently
issued the first-ever paediatric AD guidelines, highlighting prevention
strategies and a stepwise approach of effective treatments including recently
FDA approved topical therapies such as roflumilast, ruxolitinib and tapinarof
creams12 (Figure 2).
5. Modulation of
Skin Microbiome
Imbalances in the
skin microbiome are often observed in AD. Unhealthy dietary patterns, such as
those high in processed foods or low in essential nutrients (e.g., folate,
vitamin D) may lead to systemic inflammation, gut dysbiosis and innate immune
dysregulation, both resulting in a reduced production of essential
antimicrobial peptides (AMPs) by keratinocytes, skin dysbiosis and
susceptibility to skin infections. In particular, colonization with the common
bacteria Staphylococcus aureus (S. aureus)
is more frequent in severe AD. Approximately
30-60 % of AD patients have alpha toxins produced by S. aureus and its various strains that trigger immune
system responses causing inflammation, itch and sometimes infection13.
Unfortunately, there is an increased prevalence of AD skin infections caused by
methicillin-resistant S. aureus (MRSA),
which is difficult to eliminate and can become life-threatening14.
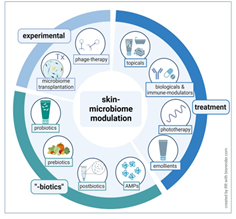
Restoring the skin microbiome can be achieved by topical and systemic
treatments for AD as well as through dietary products such as probiotics,
modulation of skin-pH and microbiome-based treatments, all of them are
considered a promising approach for personalized treatment15 (Figure 3). Supplementation
with vitamin D and vitamin E has also been shown to help reduce AD symptoms16,17. However, a
systemic review on dietary supplements including fish oil, vitamin D or vitamin
E found no convincing evidence of the benefit of dietary supplements in AD18.
Figure 3:
Modulation of skin microbiome by different therapeutic approache15.

6. Approved Systemic Therapies
An overview of systemic
therapies already approved or established in the management of patients with
moderate-to severe AD in Europe and in the USA is given in (Table 2).
Table 2: Systemic therapies for adults, children and
adolescents with moderate-to-severe atopic dermatitis.
|
Product Class/Product |
Approval Year EMA/FDA |
Standard Dosing Regimen |
Intensified Dose Regimen |
|
Conventional Systemic Immunosuppressants (Generics) |
|||
|
Cyclosporine
|
2013 (EMA) Off-label (FDA) |
2.5-5 mg/kg per day in two single oral doses for 2-8
weeks |
5 mg/kg per day in two single oral doses for up to 1
year |
|
Methotrexate* |
Off-label |
5-15 mg/ week PO or SC |
Up to 25 mg/ week PO or SC |
|
Azathioprine |
Off-label |
0.5-3 mg/kg per day based on TPMT genotype for a
period of 3 months Note: Patients with allele variants TPMT*2, *3A, *3B
and *3C have low TMPT activity are at higher risk for toxic side effects
[117]Brockmöller & Tzvetkov, 2008]. The dose must be adjusted to TPMT activity. Patients with no TPMT
activity must not receive azathioprine. |
|
|
Corticosteroids |
Unspecific license |
Due to their side effects oral steroids should only
be used up to 1 mg/kg per day for short periods of time
(only rescue therapy) |
|
|
Biologics |
|||
|
Dupilumab (Dupixent®) |
2017 (EMA) 2017 (USA) |
Adults: 600 mg SC on day 1 followed by 300 mg SC
Q2W. Remission is expected after 4-6 weeks. Children > 6 months and
adolescents: Weight based dosing regimens. Discontinuation in case no
remission is achieved after 16 weeks. |
In case of partial response after 16 weeks,
continuation with 300 mg SC Q2W can be considered. |
|
Tralokinumab (Adtralza®) |
2021 (EMA) 2021 (FDA) |
Adults and adolescents > 12 years: 600 mg SC on
day 1 followed by 300 mg SC Q2W. Remission is expected after 4-8 weeks.
Discontinuation in case no remission is achieved after 16 weeks. |
In case of partial response after 16 weeks,
continuation with 300 mg SC Q2W can be considered. |
|
Lebrikizumab (Ebglyss®) |
2023 (EMA) 2024 (FDA) |
Adults and adolescents > 12 years and ≥40 kg body
weight: 500 mg SC on day 1 and day 15 followed by 250 mg SC Q2W. Remission
expected after 4-6 weeks, then maintenance dose of 250 mg SC Q4W. Discontinuation
in case no remission is achieved after 16 weeks. |
In case of partial response after 16 weeks,
continuation with 250 mg SC Q2W up to week 24 can be considered. |
|
Nemolizumab (Nemluvio®) |
2024 (FDA) 2025 (EMA) |
Adults and adolescents > 12 years and ≥ 30 kg
body weight: 60 mg SC on day 1 followed by 30 mg SC Q4W for 16 weeks.
Discontinuation in case no remission is achieved after 16 weeks. |
In case of (partial) remission after 16 weeks
continuation with 30 mg SC Q8W can be considered. |
|
JAK-Inhibitors |
|||
|
Baricitinib* (Olumiant®) |
2020 (EMA)
Off-label (FDA) |
Adults, adolescents and children > 2 years and ≥
30 kg body weight: 4 mg QD PO (2 mg QD PO for children <30 kg body weight
and for patients with higher risk for VTE, MACE and malignancy, for patients
aged ≥ 65 years and for patients with a history of chronic or recurrent
infections). Remission expected after 1-2 weeks, then maintenance dose of 2
mg QD PO. |
If disease control is not maintained after dose
reduction, re-treatment with 4 mg QD PO can be considered. Discontinuation in case no remission is achieved
after 8 weeks of treatment. |
|
Abrocitinib* (Cibinqo®) |
2021 (EMA) 2022 (FDA)
|
Adults and adolescents > 12 years: 100 mg or 200
mg QD PO (based on individual patient risk for VTE, MACE and malignancy).
Remission expected after 1-2 weeks, then maintenance dose of 100 mg QD PO.
Discontinuation in case no remission is achieved after 24 weeks of treatment. |
If disease control is not maintained after dose reduction,
re-treatment with 200 mg QD PO can be considered. |
|
Upadacitinib* (Rinvoq®) |
2021 (EMA) 2022 (FDA)
|
Adults and adolescents > 12 years: 30 mg QD PO
(15 mg QD PO for patients with body weight < 30 kg or higher risk for VTE,
MACE and malignancy, for patients aged ≥ 65 years). Remission expected after
1-2 weeks. The lowest effective maintenance dose should be used to maintain
disease control. Discontinuation in case no remission is achieved after 3
months of treatment. |
|
|
* Contraindicated in pregnancy and lactation.
Abbreviations: BID = twice daily, IV = intravenous, JAK = Janus kinase, MACE
= major cardiovascular events, PO = per os, QD = once daily, Q2W = every 2
weeks, Q4W = every 4 weeks, Q8W = every 8 weeks, SC =subcutaneous, TMPT =
Thiopurin-S-Methyltransferase, VTE = Venous thromboembolism |
|||
6.1. Monoclonal antibodies
Dupilumab is a recombinant human IgG4 monoclonal antibody that
inhibits interleukin-4 (IL-4) and interleukin-13 (IL-13) signalling. The TH2
cytokines IL‐4 and IL‐13 interact with heterodimeric IL‐4 receptor (IL‐4R) complexes triggering transphosphorylation and
transactivation of the JAK/STAT signalling pathway, which is a key driver of
acute and chronic inflammatory processes in AD. Dupilumab can inhibit IL-4
signalling via the Type I IL-4R (IL-4Rα/γc) and both IL-4 and IL-13 signalling
through the Type II receptor (IL-4Rα/IL-13Rα1) depending on the abundance of
the IL‐4Rα and IL‐13Rα1 subunits in the target cells19.
Dupilumab was approved by EMA (2017) as Dupixent® for adults with
moderate-to-severe AD to be administered 300 mg every 2 weeks based on the SOLO
clinical trial program20,21. In
the SOLO-CONTINUE trial, high-responding patients treated with dupilumab in
SOLO were rerandomized 2:1:1:1 to continue their original regimen of dupilumab,
300 mg, weekly or every 2 weeks or to receive dupilumab, 300 mg, every 4 or 8
weeks or placebo for 36 weeks. However, longer dosage intervals and placebo
resulted in a diminution of response for all end points. Hence, the approved
regimen of 300 mg of dupilumab every 2 weeks is recommended also for long-term
treatment22. Conjunctivitis is a
common side effect of dupilumab, with incidence rates ranging from
7.9% to 19.4%in adults and from 4.8 to 14.8% in paediatric
populations23. Therefore, patients receiving dupilumab
should be monitored for ocular symptoms and
appropriate management should be provided.
Stapokibart (CM310) is a humanized monoclonal antibody
which similar to dupilumab is targeting the IL-4 receptor-α subunit (IL-4Rα), a
shared receptor for IL-4 and IL-13 which are key pathogenic drivers of AD. In
the phase 3 induction trial (NCT05265923), significant higher proportions of
adult AD patients receiving stapokibart (300 mg every 2 weeks) achieved ≥75%
improvement over placebo from baseline in EASI-75 (66.9% vs. 25.8%) and IGA
score of 0/1 with ≥2-point reduction (44.2% vs. 16.1%) at Week 16. In addition,
continued stapokibart treatment induced sustained improvements in AD signs and symptoms
without new safety signals during the maintenance treatment period over 52
weeks in adults with moderate-to-severe AD24.
Based on these positive data of the pivotal trials, the National Medicinal
Products Administration (NMPA) of China has approved stapokibart (trade
name: Kangyueda) for the treatment of adults with moderate to severe AD.
Rademikibart
(previously CBP-201) is a fully human monoclonal IgG4kappa (IgG4k) antibody blocking IL-4 receptor alpha (IL-4Rα) able
to engage fully with IL-4 and IL-13 interaction domains, including domain 1,
domain 2 and a small hinge region. It is a second-generation IL-4Rα inhibitor
that exhibits twice the binding affinity to IL-4Rα compared to dupilumab, due
to its optimized epitope design25.
In the pivotal trial (NCT05017480, SEASIDE CHINA), a significant percentage of
patients with moderate-to-severe AD who were treated with rademikibart 300 mg
every 2 weeks reached all primary and secondary endpoints (e.g., vIGA 0/1,
EASI, PP-NRS) at week 1626. Most
patients with response at Week 16 maintained them through Week 5227,28. Based on these positive results, the
Chinese National Medical Products Administration (NMPA) approved rademikibart
for the treatment of adults with moderate to severe AD in July 2025.
Tralokinumab is a fully
human IgG4 monoclonal antibody that binds to IL-13 with exceptionally high
affinity, which prevents the interaction of IL-13 with the IL-13Rα1 and with
the heterodimer IL-13 Rα1/IL-4Rα but not with the IL-13Rα2. Thus, any IL-13
that is not bound by tralokinumab (i.e., free IL-13) can be bound by IL-13Rα2
and subsequently internalized, regardless of the presence of tralokinumab29. Tralokinumab was approved by EMA (2021)
as Adtralza® for the treatment of moderate-to-severe AD in adults based on the
data of the phase 3 program (ECZTRA 1, ECZTRA 2 and ECZTRA 3 trials). In
the two identical ECZTRA 1&2 trials, tralokinumab 300 mg Q2W was
significantly superior to placebo with respect to improvements in primary
endpoints IGA 0/1 and EASI-75 after 16 weeks and secondary endpoints in the
16-week analysis (including pruritus scores, DLQI, SCORAD, EASI-50 and EASI-90
and eczema-related sleep interference)30.
The ECZTRA 3 trial was designed based on real-world experience as it introduced
systemic therapy with tralokinumab 300 mg every two weeks in combination with
mometasone furoate 0.1 % cream (once daily to active lesions as needed) in
moderate to severe AD patients who were inadequately controlled by topical
therapy and systemic corticosteroids. This combination of tralokinumab and
topical mometasone furoate improved EASI-75 and IGA 0/1 at week 16
significantly compared with placebo: 56.0 versus 35.7 % (P < 0.001) and 38.9
versus 26.2 % (P = 0.015), respectively. Clinical benefits were also reported
for secondary endpoints at week 16 such as EASI-90 (32.9 versus 21.4 %; P =
0.022) and EASI-50 (79.4 versus 57.9 %; P < 0.001)31.
Lebrikizumab is an IgG4
monoclonal antibody that binds with high affinity to interleukin IL-13 and
selectively inhibits IL-13 signalling through the IL-4 receptor alpha (IL-4Rα)/
IL-13 receptor alpha 1 (IL-13Rα1) heterodimer, thereby inhibiting the
downstream effects of IL-13. Lebrikizumab does not prevent the binding of IL-13
to the IL-13Rα2 (decoy receptor), which allows the internalisation of IL-13
into the cell. In 2023, the EMA approved lebrikizumab (EbGLYSS®) for the
treatment of moderate-to-severe AD in adults and adolescents aged 12 and older,
weighing at least 40 kg, who are candidates for systemic therapy32. The market authorisation was given due to the results
of the ADVOCATE program including three phase 3 trials. In the first study, involving 424 patients with AD, 43% of patients who
received lebrikizumab achieved an IGA score of 0 or 1 compared with 13% of
patients who received placebo. In addition, 59% of patients achieved EASI-75
with lebrikizumab compared with 16% of patients on placebo. In the second
study, involving 445 patients with AD, 33% of patients had an IGA score of 0 or
1 with lebrikizumab compared with 11% of patients on placebo. In addition, 52%
of patients receiving lebrikizumab achieved EASI-75 compared with 18% of
patients receiving placebo. In the third study, involving 228 AD patients who
were also given topical corticosteroids, 41% of patients given lebrikizumab and
corticosteroids had an IGA score of 0 or 1 and 70% achieved EASI-75. The
results for patients given placebo and corticosteroids were 22% and 42%
respectively. In terms of long-term treatment, the beneficial effect of
lebrikizumab was maintained up to 52 weeks in patients who achieved IGA 0
or 1 and EASI-75 at week 16. The most common side effects with lebrikizumab (which
may affect up to 1 in 10 people) include injection site reactions, dry eye and
conjunctivitis including allergic conjunctivitis33.
Long-term studies of up to 3 years report sustained efficacy and a consistent
safety profile and tolerability over time34.
Nemolizumab is a
humanised IgG2 monoclonal antibody that inhibits interleukin-31 (IL-31)
signalling by binding selectively to IL-31 receptor alpha (IL-31Rα). IL-31 is belonging to the IL-6 cytokine family and is deriving from TH2 cell responses. The IL-31 receptor is a heterodimer, consisting of the
IL-31Rα chain and oncostatin M receptor β-chain (OSMR-β). IL-31 induces a signal transduction pathway through
the JAK/STAT, phosphatidylinositol 3-kinase (PI3K) and mitogen-activated protein
kinase (MAPK) pathways35. It is involved in the underlying mechanisms of AD and
specifically associated with pruritus, inflammation, epidermal dysregulation
and fibrosis36-38. In AD clinical trials, nemolizumab was found to modulate gene
expression related to the pathophysiology of AD by decreasing the inflammatory
and proliferative profile of T-cells and monocytes/macrophages without leading
to immunosuppression. In February 2025, the European Commission approved
nemolizumab as Nemluvio® for moderate to severe AD in patients aged 12 years
and older due to its effectiveness demonstrated in the phase 3 ARCADIA program
with the advantage of once monthly dosing compared to twice monthly dosing
required for dupilumab, lebrikizumab and tralokinumab39: ARCADIA 1 and ARCADIA 2 enrolled a total
of 1728 subjects 12 years of age and older with moderate-to-severe atopic
dermatitis not adequately controlled by topical treatments. Disease severity
was defined by an IGA score of 3 (moderate) and 4 (severe), an EASI score of at
least 16, a minimum BSA involvement of 10% and a PPNRS score of at least 4.
Subjects in the studies received initial subcutaneous (SC) injections of either
nemolizumab 60 mg, followed by 30 mg injections every 4 weeks or matching
placebo. Nemolizumab was statistically significant superior to placebo with
respect to skin-related co-primary endpoints IGA success (score of 0 or 1 with
≥2-point improvement) and EASI-75 over 16 weeks. Results for both co-primary
endpoints were consistent in the severe pruritus population (baseline PPNRS ≥
7) (Figure 4). The most common side effects with nemolizumab included hypersensitivity
reactions and injection site reactions. Formation of anti-drug-antibodies was
frequently observed, but without affecting its pharmacokinetics, safety or
efficacy. In the ARCADIA long-term extension trial (NCT03989206), treatment
with 30 mg nemolizumab every 4 weeks maintained significant and progressive
improvements in disease activity, itch, sleep and quality of life for up
to 104 weeks. The safety profile of nemolizumab remained stable, with no new
safety signals observed40.
Figure 4: Coprimary endpoints in ARCADIA 1 and ARCADIA 2.

Non-responder
imputation analysis was used. Adjusted effect sizes (percentage difference with
97·5% CIs) and p values versus the placebo group are from a Cochran–
Mantel–Haenszel test adjusting for the randomisation stratification variables.
EASI=Eczema Area and Severity Index. IGA=Investigator’s Global Assessment.
n=number of participants with data after imputation. PP-NRS=Peak Pruritus
Numerical Rating Scale. TCI=topical calcineurin inhibitors. TCS=topical corticosteroids39.
7. JAK Inhibitors
The Janus kinase
(JAK)/signal transducers and activators of transcription (STAT) pathway play a
crucial role in cytokine signalling and regulates the functions of TH1, TH2, TH17
and TH22 cells, which are involved in the inflammatory pathogenesis of AD. The JAK
family of enzymes consists of four members, JAK1, JAK2, JAK3 and tyrosine
kinase 2 (TYK2) which work in pairs to phosphorylate and activate one or more
of the seven transcription factors of the STAT family (STAT1, STAT2, STAT3,
STAT4, STAT5A, STAT5B and STAT6) which modulate gene expression and cellular
functions. The TH2 cytokines IL-4, IL-13 and IL-31 are signalling via
transmembrane receptors coupled to the JAK/STAT pathway and are also driving
itch, the main symptom of AD. TYK2 acts as an intracellular signalling enzyme
and is crucial for signalling pathways of IL-12/Th1/, IL-23/Th17, as well as
type I IFN cell responses and may provide new alternatives for AD treatment5. Since JAK inhibitors are small molecules
that can be taken orally, they work faster to relieve symptoms, especially
itching, compared to some other treatments. Unlike monoclonal antibodies that
target only one or two specific cytokines, JAK-inhibitors block multiple
signalling pathways at once, making them highly effective against a wide range
of inflammatory signals in AD. By achieving a broad, intermittent inhibition of
the activity of multiple cytokines, JAK inhibitors help to modulate TH2
cell-mediated inflammation, epidermal barrier dysfunction and itch signalling.
This comprehensive blockade, however, can affect essential immune functions,
which may lead to an increased risk of severe infections. In addition, FDA
still requires warnings about an increased risk of serious heart-related
events, cancer, blood clots and death for JAK inhibitors in the treatment of
inflammatory conditions including AD41. The warning was prompted primarily from
tofacitinib studies in rheumatoid arthritis, an assumed class effect and the
absence of long-term safety data for recently approved oral JAK-inhibitors. At
present, three systemic oral JAK-inhibitors including baricitinib, abrocitinib
and upadacitinib have received approval for systemic use in moderate to severe
AD whereas ruxolitinib and delgocitinib have been recently approved for topical
AD treatment42 (Figure 5).
Figure 5: Mechanism of action of approved JAK inhibitors.

JAK inhibitors inhibit
different combinations of JAK intracellular proteins. Upon binding of a
cytokine to its receptor, intracellular JAK proteins mediate recruitment and
tyrosine phosphorylation of STAT proteins. Phosphorylated STAT proteins
dimerize and translocate to the nucleus, where they regulate different genes.
Abbreviations: IFN =
interferon gamma, IL = interleukin, JAK = Janus kinase, STAT = signal
transducer and activator of transcription, TYK2 = tyrosine kinase 242.
Baricitinib (Olumiant®)
is a selective and reversible inhibitor of JAK1 and JAK2 thereby reducing the
phosphorylation and activation of STATs. In the pivotal
phase 3 study (BREEZE-AD7), baricitinib in combination with topical corticosteroids showed significant effects
compared to placebo for the primary endpoints at week 16: a vIGA for AD
score of 0 (clear) or 1 (almost clear) was achieved by 31% of patients
receiving 4 mg of baricitinib, 24% receiving 2 mg of baricitinib compared with
15% receiving placebo, all three groups received also topical corticosteroid
therapy43. Baricitinib was the first
systemic JAK1/JAK2 inhibitor approved by EMA in 2020 for the treatment of
mild-to-moderate AD. Except the USA, it has been approved for treating moderate‐to‐severe AD in
adult patients in more than 70 countries and in over 30 countries for
adolescents and children from age 2 years with moderate‐to‐severe AD, who
are candidates for systemic therapy44. In 2024, a final integrated safety analysis of
baricitinib therapy in moderate-to-severe AD was published, including data from
eight trials from the BREEZE program with a duration of up to 200 weeks,
resulting in a maximum exposure of 4.6 years of therapy. Rates of major adverse
cardiovascular events, deep vein thrombosis/pulmonary embolism, malignancies
and serious infections were within ranges of background rates in patients with
AD. These outcomes continue to demonstrate a consistent and well‐established safety profile for baricitinib, with no
new safety signals45.
Abrocitinib (Cibinqo®)
is a selective JAK1 inhibitor preventing the phosphorylation and activation of
STATs. Abrocitinib showed significant efficacy
compared to placebo in the JADE (JAK1 Atopic Dermatitis Efficacy and
Safety) clinical phase 3 program, which consisted out of the JADE MONO-1 (NCT03349060)
and the JADE MONO-2 (NCT03575871) trials in subjects aged 12 years and older
with moderate to severe AD46,47. In
addition, in the active comparator trial JADE COMPARE (NCT03720470) abrocitinib
was tested against placebo or dupilumab in adult subjects with moderate to
severe AD on background topical therapy48:
The two primary endpoints at Week 12 were met: (i) proportion of patients
achieving an IGA score of 0 (clear) or 1 (almost clear), with an improvement
from baseline (IGA 0/1) and (ii) the proportion of patients achieving
improvement in the EASI-75 score. The key secondary endpoint was the proportion
of patients achieving point improvement on the Peak Pruritus Numerical Rating
Scale (PP-NRS) at Week 2 and Week 12, demonstrating a rapid and substantial
reduction in itch compared to placebo. Treatment with abrocitinib at a dose of
either 200 mg or 100 mg once daily resulted in significantly greater reductions
in signs and symptoms of moderate-to-severe AD than placebo at weeks 12 and 16.
The 200-mg dose, but not the 100-mg dose, of abrocitinib was superior to
dupilumab with respect to itch response at week 2. Neither abrocitinib dose
differed significantly from dupilumab with respect to most other key secondary
end-point comparisons at week 16.
Upadacitinib
(Rinvoq®) is a selective and
reversible JAK1 inhibitor. In human cellular assays, upadacitinib selectively
inhibits signalling by JAK1 and JAK1/3 with functional selectivity over
cytokine receptors that signal via pairs of JAK2. Inhibiting JAK1 with
upadacitinib reduces the signalling of many mediators which drive the signs and
symptoms of AD such as eczematous skin lesions and pruritus. The efficacy and
safety of upadacitinib 15 mg and 30 mg once daily has been demonstrated in
three phase 3 studies (MEASURE UP 1, MEASURE UP 2 and AD UP) in adult and
adolescent patients with moderate to severe AD not adequately controlled by
topical medications. A significantly greater proportion of patients treated
with upadacitinib 15 mg or 30 mg achieved vIGA-AD 0 (clean) or 1 (almost
clean), EASI 75 or a ≥ 4-point improvement on the Worst Pruritus NRS compared
to placebo at week 16. Rapid improvements in skin clearance and itch were also
achieved49.
8. Approved Topical Therapies
Most topical treatments for AD are generic products such
as topical corticosteroids (TCS) and topical calcineurin inhibitors (TCI). TCS
are used for short-term treatment of inflammatory flare-ups, while TCI are an
alternative, especially for sensitive skin areas. New developments include
topical JAK inhibitors and phosphodiesterase 4 (PDE4) inhibitors, which have demonstrated
significant results in both adult and paediatric patients whilst possessing a
favourable safety profile. The JAK inhibitors ruxolitinib and delgocitinib and the
PDE4 inhibitors crisaborole, roflumilast and difamilast have already received
approval as topical AD treatments by the US-FDA and/or the Japanese
Pharmaceuticals and Medical Devices Agency (PMDA) but not by the EMA. The
American Academy of Dermatologists strongly recommends topical treatment of inflamed
areas with ruxolitinib cream for children older than 12 years with mild-to-severe
AD as it effectively decreases the severity of the dry and itchy skin. An
overview of topical therapies which have been already approved or established
in the management of patients with atopic dermatitis is given in (Table 3).
Table 3: Approved topical
treatments for adults, children and adolescents with AD.
|
Topical
Product |
Approvals EMA/FDA/PMDA
|
Dosing
Recommendations |
|
Corticosteroids |
|
|
|
Topical Corticosteroids with different therapeutic index |
More than 30 generic products for skin diseases
including AD |
In general, TCS only for treatment
of acute flares for a short period of time: ·
Potent to very potent
TCS for adolescents and adults and children up to 2
years under specialist supervision ·
Low
to moderate potency TCS can routinely be used for patients ≥ 2
years. ·
For children < 2
years, any TCS treatment should be under specialist supervision. |
|
Calcineurin Inhibitors |
|
|
|
Tacrolimus |
Several generic products for moderate to
severe AD when TCS treatment is not sufficient or not possible |
·
Tacrolimus 0.03%
ointment for adults and children ≥ 2 years ·
Tacrolimus 0.1%
ointment for patients ≥16 years |
|
Pimecrolimus |
Several generic products for mild to
moderate AD when TCS treatment is not sufficient or not possible |
·
Pimecrolimus 1% cream
for patients aged 3 months and older |
|
JAK-Inhibitors |
|
|
|
Ruxolitinib
|
FDA (2020): OPZELURA® approved for mild to moderate AD
in adults
FDA (Sep 2025): OPZELURA® approved for AD in children |
·
1.5% cream for adults and adolescents
(≥12 years) to be applied twice daily -up to 20 % BSA (not more than 60 gram
per week)
·
1.5% cream for children 2-11
years to be applied twice daily (not more than 60 gram per 2 weeks) |
|
Delgocitinib
|
PMDA (2020): CORECTIM®
for adult
and paediatric AD
EMA (2024): ANZUPGO® for moderate to severe hand eczema |
·
0.5 % ointment for
adults twice daily (not exceeding 5 g at a time) ·
0.25% ointment for
children to be applied twice daily (not exceeding 5 g at a time)
·
2% cream for adults with
hand eczema twice daily on affected skin of hands and wrists up to 12 weeks |
|
PDE4 Inhibitors |
|
|
|
Crisaborole
|
FDA (2016): EUCRISA™ for adults, adolescents and children ≥ 2 years with ≤ 40% affected body
surface area (BSA)
EMA (2020): STAQUIS® Not
marketed in EU due to withdrawal of MA by EC on request of Pfizer in 2022 |
·
2% ointment to be used twice
daily up to 12 weeks |
|
Difamilast
|
PMDA (2021): MOIZERTO® for adult and paediatric AD FDA (February 2026): ADQUEY™ for mild to moderate AD |
·
1% ointment for adults and
children ≥ 2 years twice daily ·
1% ointment for adults and
children ≥ 2 years twice daily |
|
Roflumilast
|
FDA (2024): ZORYVE® for adult and paediatric AD |
·
0.15% cream for patients
aged 6 years and older to be applied once daily ·
0.05% cream for children
aged 2-5 years to be applied once daily |
|
Aryl hydrocarbon receptor agonist |
|
|
|
Tapinarof
|
FDA (2024): VTAMA™ for patients aged 2 years and older with AD |
·
1% cream to be applied to
affected areas once daily |
Abbreviation: AhR = aryl
hydrocarbon receptor, EC = European Commission, JAK = Janus Kinase, PDE4 =
Phosphodiesterase 4, PMDA = Pharmaceuticals and Medical Devices Agency (Japan).
Source: Based on
European and US American guidelines for the management of atopic dermatitis10-12 and the SMPCs of
ANZUPGO®67, ZORYVE®75, VTAMA™79, OPZELURA®122, EUCRISA™123, ADQUEY™124 and the drug
information sheet of CORECTIM®125.
8.1. Topical Corticosteroids
(TCS)
TCS have been the cornerstone of AD treatment for 40
years. Hydrocortisone was the first agent to be used; since then, around 30
other corticosteroid preparations have been approved for AD treatment. TCS are
considered a first line treatment to reduce inflammation, pruritus and relapses
and act for AD flares after basic management with moisturizers50,10. Corticosteroids
are lipophilic and therefore penetrate the skin well where they bind to the
steroid receptor in the cytoplasm of keratinocytes and fibroblasts within the
epidermis and dermis. The corticosteroid-receptor complex translocates to the
nucleus where it binds to the glucocorticoid-response element (a specific
sequence of DNA) thereby inducing anti-inflammatory and metabolic proteins -
called transactivation. In addition, corticosteroid molecules can interact
directly or indirectly with regulatory genes for inflammation thereby
downregulating proinflammatory transcription factors - called transrepression.
TCS induced genomic (transactivation and transrepression) processes as well as
non-genomic processes (vasoconstrictive effects) result in strong
anti-inflammatory, anti-proliferative (antimitotic) effects but may also
downregulate immune responses and inhibit T lymphocyte functions51 (Figure 6).
Figure 6: Genomic and
non-genomic mechanisms of action of topical corticosteroids51.

TCS were originally classified only by their potency
based on the skin vasoconstriction assay, which measures skin blanching on
topical application52,53. Most European countries are
using the classification according to Niedner from mild (class I) to
super-potent corticosteroids (class IV)54 while the WHO classification
allocates 7 groups starting from VII (weakest) to I (most potent)55 which is used by
US-American dermatologists. Today, TCS are classified by potency and
the risk of side effects such as atrophy, striae, rosacea, teleangiectasias,
purpura and other cutaneous and systemic reactions. A therapeutic index (TIX)
has been introduced for TCS based on a concept of the benefit-risk ratio
evaluation concerning both efficacy and safety56. The TIX is the ratio of desired
versus adverse effects of the TCS. Since a TIX of 1–2 is defined as an equal
relation of desired and adverse effects, a TIX of 2-3 indicates a TCS with
improved benefit-risk ratio. For example, mometasone furoate, a class III corticosteroid
with a TIX of 2 has stronger desired effects than adverse effects57 (Table 4).
Table 4: Classification
of TCS based on therapeutic indices and their potential to induce skin atrophy.
TIX |
Skin atrophy |
Class |
Glucocorticoid |
|
1 |
1 |
I |
Hydrocortisone |
|
1.06 |
2 |
II |
Triamcinolone acetonide |
|
1.2 |
2 |
III |
Betamethasone valerate |
|
1.4 |
1 |
II |
Hydrocortisone butyrate |
|
1.5 |
2 |
IV |
Clobetasol
propionate |
|
2 |
1 |
II |
Prednicarbate |
|
2 |
1 |
II |
Methylprednisolone aceponate |
|
2 |
1 |
III |
Mometasone furoate |
Class: I, weak; IV,
very strong. TIX, therapeutic index: 1 ≤2 relation between desired and adverse
effect is equal, 2-3 GC with improved benefit/risk ratio. Skin atrophy: 1, GC
induces little skin atrophy; 2, GC induces much skin atrophy57.
Low and medium potency TCS can be used for a longer
duration with reduced atrophy risk compared to higher potency TCS. High and
very high potency TCS should only be used to treat severe AD flares. The latest
generation TCS with innovative vehicles such as nanocarrier show an improved
pharmacokinetics and a better risk-benefit ratio and are therefore favoured
over earlier generation TCS. Modern, double-esterified TCS (hydrocortisone
butyrate, hydrocortisone aceponate, hydrocortisone butyrate, prednicarbate,
methylprednisolone aceponate, mometasone furoate) have a pronounced
anti-inflammatory effect but no strong antiproliferative properties with less
potential for skin atrophy57,58. For the treatment of the
face and neck, only weak to moderately potent corticosteroids should be used and
for a few days only. TCS are usually applied in the ranges from twice weekly to
once or twice daily for a two-week period.
9. Topical Calcineurin Inhibitors (TCI)
TCI such as tacrolimus and pimecrolimus have also immunosuppressive
effects and inhibit T lymphocyte activation, but penetrate the skin less than
corticosteroids. Therefore, they are the preferred treatment for sensitive skin
areas such as face and neck. The anti-inflammatory effect of 0.1% tacrolimus
ointment is comparable to that of a medium-strong TCS or 1% pimecrolimus cream59.
9.1. Topical JAK Inhibitors
(TJI)
TJI reduce signalling of key inflammatory cytokines
such as IL-4, IL-13 and IL-31 involved in the pathogenesis of AD. Delgocitinib and
ruxolitinib are effective in treating AD and significantly improved EASI, IGA,
pruritus-NRS score in late phase clinical trials with adult AD patients. All
topical JAK inhibitors show minimal risk of mild-to-moderate adverse effects.
Ruxolitinib (Opzelura®) is a topical JAK1/2-inhibitor that has shown similar or even higher efficacy in adults with mild-to-moderate
AD compared to triamcinolone cream (group III TCS) and has been approved by the US-FDA for its use in the
treatment of AD60. The 2023 AAD guidelines have given a strong
recommendation for topical JAK inhibition with ruxolitinib 1.5% cream for mild
to moderate AD in patients at least 12 years of age and up to 20% affected BSA
without any topical drug interaction warning50. In 2024, the American Academy of Allergy, Asthma and
Immunology (AAAAI) recommended topical ruxolitinib as effective for AD patients
unresponsive to conventional therapies or with contraindications to systemic
immunosuppressants61. An updated systematic review and meta-analysis of
five randomized clinical trials that enrolled patients predominantly with
moderate-to-severe AD concluded that monotherapy with ruxolitinib cream does significantly improve
moderate-to-severe AD, without a significant increase in adverse events across
all age groups62.
Delgocitinib (Anzupgo®) is a topical JAK1/2/3/TYK2
(pan)JAK-inhibitor which significantly improved pruritus
and EASI in adult Japanese patients with moderate to severe AD63. Moreover, topical
delgocitinib was observed to have a great efficacy in the treatment of AD in
children in Japan64. In 2020, the Japanese PMDA
approved delgocitinib for adult and paediatric AD patients as 0.5% and 0.25% CORECTIM® ointment,
respectively. In the European Union, delgocitinib has been approved
as a 2% creme
(Anzupgo®) for the treatment of moderate to severe chronic hand eczema in
adults for whom topical corticosteroids are not sufficient or are not suitable.
The approval was based on the positive safety and efficacy outcomes of three
phase 3 trials: adults with moderate to severe chronic hand eczema received
twice-daily 2% delgocitinib cream or cream vehicle for 16 weeks (DELTA 1&2)
and up to 52 weeks in the open-label extension trial (DELTA 3). The primary
endpoint was the Investigator’s Global Assessment for Chronic Hand Eczema
(IGA-CHE), defined as IGA-CHE score of 0 (clear) or 1 (almost clear, defined as
only barely perceptible erythema), which was met at week 16 and week 52, respectively65,66. The safety and efficacy of Anzupgo® in
children and adolescents under 18 years of age have not been established so far67.
10. Topical PDE4 Inhibitors (TPI)
Several TPI have been already approved for treatment
of adult and paediatric patients with mild to moderate AD by the US-FDA
(crisaborole, roflumilast and difamilast) and by the Japanese PMDA
(difamilast). None of these TPI has currently a marketing authorisation in the
European Union. The inhibition of PDE4 increases intracellular cyclic adenosine
monophosphate (cAMP) levels. Drugs that elevate intracellular cAMP
levels suppress immune functions of T cells, monocytes, macrophages and
neutrophils, by reducing the production of pro-inflammatory cytokines and by
increasing the production of anti-inflammatory mediators68 (Figure 7).
Figure 7: Immunomodulatory
action of PDE4-inhibitors.

PDE4 inhibitors suppress inflammatory immune responses
by elevating intracellular cAMP levels. Increased level of cAMP inhibits the
production of pro-inflammatory cytokines through simultaneous inhibition of
PKA-NFkB and Epac1/2-NFkB pathways; and promotes the production of
anti-inflammatory mediators by activation of the PKA-CREB pathway. The
intracellular level of cAMP is mainly controlled by the activity of adenylyl
cyclase and PDE4. Abbreviations: adenylyl cyclase = AC, phosphodiesterase 4 =
PDE4, protein kinase A = PKA, exchange protein 1/2 activated by cAMP = Epac1/2,
phosphorylated cAMP-responsive element binding protein = pCREB, nuclear factor
kappa-light-chain-enhancer of activated B cells (NFkB), inhibitor of PDE4 =
PDE4i68.
Crisaborole is a medium potent, selective PDE4
inhibitor (especially of the PDE4A subtype). It is a low molecular weight boron
compound with a non-steroidal structure. Due to its small size, the active
ingredient can penetrate the upper layers of the skin. In 2016, crisaborole 2 %
ointment has been approved as EUCRISA™ by the US-FDA for treatment of mild to
moderate AD in patients 2 years of age and older. The approval of EUCRISA™ is
based on two phase 3 trials in which adult and paediatric patients with mild to
moderate AD received either crisaborole 2% ointment or vehicle twice daily for
28 days. In both trials, the primary efficacy endpoint [improvement of the
Investigator’s Static Global Assessment (ISGA) score of 0 (clear) or 1 (almost
clear) with at least a 2-grade improvement from baseline at day 29] was met.
Moreover, crisaborole demonstrated a favourable safety profile and reduction in
overall disease severity, pruritus and other signs of AD69. Crisaborole has been
approved in the European Union in 2020 but is not commercialized in Europe
since the European Commission has withdrawn its marketing authorisation in 2022
at the request of the marketing authorisation holder, Pfizer Europe MA
EEIG, which notified the European Commission of its decision not to market the
product in the EU for commercial reasons.
Difamilast is a PDE4 inhibitor (especially of the
PDE4B subtype) exerting mainly anti-inflammatory action by reducing
inflammatory cytokines like TNFα and more effectively than other
PDE4-inhibitors (CP-80633, cipamfylline and crisaborole)70. In the phase 3
program, 0.3% and 1% difamilast ointment twice
daily has shown significant improvements compared to vehicle in the EASI and
IGA scores in Japanese adult and paediatric AD patients at week 471,72 and up to
52-weeks73. In 2021, the
Japanese PMDA approved 1% difamilast ointment as MOIZERTO® for the treatment of
AD. In February 2026, the US-FDA has approved 1% difamilast ointment as ADQUEY™
for the treatment of mild-to -moderate AD in patients of 2 years of age and
older.
Roflumilast is a highly potent PDE4-inhibitor without
any particular selectivity for the various PDE4 isoforms (i.e., a
pan-PDE4-inhibitor). In 2024, roflumilast received FDA approval as ZORYVE®
0.15% cream based on the results of two phase 3 vehicle-controlled studies
(INTEGUMENT-1 and INTEGUMENT-2), which evaluated 1337 patients with mild to
moderate AD ages 6 years and older. Patients applied ZORYVE cream 0.15% or
vehicle once daily for 4 weeks. The primary endpoint (vIGA-AD at week 4) and the
secondary endpoint (Peak Pruritus-NRS at week 4) were met. Roflumilast improved
AD relative to vehicle cream, based on multiple efficacy end points, with favourable
safety and tolerability74. In the following, a
roflumilast 0.05 % cream has been approved for children in the age of 2-5 years
based on the results of the phase 3 INTEGUMENT-PED trial, where the cream or
vehicle was applied once daily for 4 weeks75. In March 2026,
Arcutis announced new data from the INTEGUMENT-INFANT Phase 2 trial
demonstrating that ZORYVE® cream 0.05% reduced signs and symptoms of AD in
infants aged 3 months to less than 24 months with mild to moderate atopic
dermatitis76.
11. Topical Aryl Hydrocarbon Receptor Agonist
Tapinarof (3,5-Dihydroxy-4-isopropylstilben) is a
fist-in-class, nonsteroidal small molecule agonist of the aryl hydrocarbon
receptor (AhR), which has been originally isolated from metabolites of the
bioluminescent bacterium Photorhabdus luminescens that lives symbiotic in the
gut of insect-specific pathogenic nematodes. The anti-inflammatory and
antibiotic properties of tapinarof confer a competitive advantage to organisms
producing it over other bacteria and therefore prevent rapid insect putrefactio77. The AhR is a
ligand-dependent transcription factor that plays a role in regulating cytokine
and skin barrier protein expression as well as antioxidant activity78 (Figure 8).
Tapinarof reduces TH2 and TH17 responses and modulates regulatory T cell (Treg)
functions in inflammatory skin diseases like AD and psoriasis. Tapinarof
restores the epidermal barrier through upregulation of protective proteins such
as filaggrin, hornerin and involucrin and increases antioxidant responses via direct
binding to nuclear transcription factor DNA recognition elements. In 2024, the
US-FDA approved tapinarof 1% cream as VTAMA™ for patients aged 2 years and
older with mild to severe AD. The approval was supported by positive data of
the phase 3 ADORING program demonstrating a significant improvement in the vIGA
(clear (0) or almost clear (1)) and rapid itch relief (PPNRS at least 4 points reduction) after 8 weeks (ADORING 1&2) and up to 48 weeks (ADORING 3) of treatment in
patients who received tapinarof 1% cream compared to those who received
vehicle. Tapinarof 1% cream was well-tolerated, the most commonly reported adverse effects reported in
ADORING 1&2 were upper and lower respiratory tract infection, folliculitis,
headache, asthma, vomiting, ear infection, pain in extremity and abdominal pain79.
Figure 8: Mechanisms of
action of tapinarof in skin diseases.

Abbreviations: AD = atopic
dermatitis, AhR = aryl hydrocarbon receptor, ARNT = Aryl hydrocarbon receptor
nuclear translocator, Nrf2 = nuclear factor erythroid 2–related factor-2, PsO =
Psoriasis, ROS = reactive oxygen species, Th2 = Thelper 2 cells, Th17 = Thelper
17 cells, TRM = memory resident T cells78.
11.1. Current AD drug pipeline
Management of moderate-to-severe AD needs still more effective
and safe long-term therapeutic products able to reduce recurrent flares and
disease burden. Several new drug developments are emerging including small
molecules and biologics tackling old and new targets which should diversify
therapeutic options in AD. New innovative approaches are thought to adopt better
individual patient needs and requirements including lower dosing frequency and
less side effects. The most advanced new drug developments for systemic
administration are the monoclonal antibody amlitelimab targeting the OX40/OX40L
pathway and the oral TYK2 inhibitor ICP-332. Novel promising topical therapies
include ointments of pan-JAK inhibitors including MH004, CGB-500 and LNK01004
and the antimicrobial gel zabalafin.
11.2. Monoclonal antibodies targeting the OX40/OX40L
pathway
A new potential therapeutic target in T cell-mediated
skin diseases is OX40, a receptor highly expressed on activated T cells and its
ligand OX40L (OX40/OX40L), which is mainly expressed on professional
antigen-presenting cells (APC) such as Langerhans cells, dendritic cells, B
cells, type 2 innate lymphoid cells (ILC2), fibroblasts, endothelial cells and
mast cells. Activation of the OX40/OX40L pathway in inflammatory skin enhances
effector T cell proliferation and survival, promotes the generation of memory T
cells and increases the production of pro-inflammatory cytokines resulting in
persistent skin inflammation, chronic itch and skin barrier dysfunction6. Blocking OX40/OX40L axis is expected to suppress TH2-driven
inflammation, as well as potentially inhibiting TH1, TH17 and TH22 responses.
Recent clinical trials investigate the effects of antibodies targeting OX40
(rocatinlimab and telazorlimab) or OX40L (amlitelimab) seeking to demonstrate
long-term safety and treatment efficacy in patients with moderate-to-severe AD80 (Figure 9).
Figure 9: Novel monoclonal antibodies targeting the OX40/OX40L costimulatory
signalling pathway.

Abbreviations: APC, Antigen-presenting cell; Th, T-helper; IL,
interleukin; OX40L, OX40 ligand80.
Amlitelimab (also known as KY1005 or SAR445229) from Sanofi (licensed from Kymab) is a non-T cell depleting,
non-cytotoxic fully human IgG4 monoclonal antibody that blocks the interaction
between OX40L on APCs and OX40 on T cells, effectively blocking OX40
stimulation and T-cell-mediated inflammatory responses thereby restoring the
balance between pro-inflammatory and regulatory T cells80. Positive results from the COAST 1 phase
3 study (NCT06130566) showed that amlitelimab dosed either every 4 weeks or
every 12 weeks, met all primary endpoints, demonstrating significant and
clinically meaningful skin clearance and reduced disease severity compared to
placebo at week 24 in patients aged 12 years and older with moderate to severe
AD. Recently, Sanofi announced that it already plans
regulatory filings for AD candidate amlitelimab after reporting positive data
in the COAST 2 [NCT06181435) and SHORE (NCT06224348) trials81. Phase 3 program is ongoing with trial
ESTUARY (NCT06407934) to confirm and extend the findings of COAST 1, COAST 2
and SHORE trials, that blockade of OX40L–OX40 signalling could lead to
long-term durable responses with extended dosing frequency beyond every 4 weeks
combined with a good safety profile.
Rocatinlimab (previously KHK4083 or AMG 451) from
Kyowa Kirin/Amgen is a non-fucosylated IgG1 anti-OX40 monoclonal antibody that
inhibits and reduces the number of pathogenic OX40+ T cells80. Phase 2b trials showed significant,
progressive improvements in clinical severity with a tolerable safety profile
in patients with moderate-to-severe AD compared to placebo82. Rocatinlimab was tested in the phase 3 ROCKET
program with eight trials targeting diverse populations with moderate-to-severe
AD, including adults and adolescents with inadequate response,
contraindications or intolerance to topical or systemic treatments. A recent safety update from the global ROCKET program
identified emerging concerns of malignancies with possible viral or
immune-related links. This included one new confirmed case and one suspected
case of Kaposi’s sarcoma, in addition to the previously confirmed case, suggesting
a potential mechanistic link to OX40 pathway modulation. While the overall
number of malignancy cases across the program remains below expected background
rates, the characteristics of these cases raise a plausible biological concern
that cannot be excluded. Based on this update and previously reported safety
risks, both Kyowa Kirin and Amgen have concluded that the potential risks may
outweigh the benefits for the studied patient populations and discontinued
rocatinlimab clinical trials83.
Telazorlimab (previously ISB830) from Ichnos Sciences
is a humanized anti-OX40 IgG1 monoclonal antibody80.
Telazorlimab has been evaluated in a phase 2b trial (NCT03568162) where it was SC
administered at 300mg or 600 mg every 2 weeks in patients with moderate to
severe AD. Telazorlimab treatment was well tolerated and the mean percentage
change from baseline in EASI was significantly greater in subjects receiving
telazorlimab versus placebo at week 16. The most common TEAE were exacerbation
of AD, nasopharyngitis, upper respiratory tract infection, viral infection and
headache. One patient experienced paraesthesia, considered to be related to
telazorlimab treatment and was discontinued from the study84.
IMG-007 from Inmagene LLC is a non-depleting anti-OX40
monoclonal antibody designed to silence
antibody-dependent cellular cytotoxicity (ADCC) function to minimize
potential safety risks and to have a prolonged half-life to enable potentially less frequent dosing regimen.
Single doses of IMG-007 up to 600 mg were well-tolerated in healthy subjects
and exhibited an extended mean terminal half-life up to approximately 38 days
at high doses85. In the phase 2a
open-label trial (NCT05984784) with adult patients with moderate to severe AD, a
4-weeks treatment with IMG-007 resulted in a mean reduction in EASI of 77% and
EASI-75 response of 54%, at week 16. Durable inhibition of inflammatory markers
including of TH1, TH2 and TH17 cells was observed for up to 24 weeks. IMG-007
infusions were well-tolerated with no reports of pyrexia or chills. The safety
and efficacy of various SC dosing regimens of IMG-0047 is currently evaluated
in the phase 2b trial (NCT07037901, ADAPTIVE). The primary outcome is the mean percentage change
from baseline in EASI at week 20.
11.3.
Monoclonal antibodies targeting inflammatory cytokines
APG777
from Apogee Therapeutics is a humanized
IgG1 monoclonal antibody with an optimized pharmacokinetic profile. APG777 has
high affinity to IL-13 and includes a triple amino acid modification (the “YTE”
modification) in its Fc region that is designed to extend its half-life up to 28
days. The dose-proportional systemic exposure of APG777 and positive
risk-benefit ratio established in preclinical studies support its continued
clinical development for IL-13-mediated diseases. The extended half-life of
APG777 suggests potential benefits in reducing dosing frequency compared with
existing IL-13-targeting therapies, which could improve treatment adherence and
patient outcomes86. The safety and
efficacy of APG777 are currently being investigated in the Phase 2 clinical
trial (NCT06395948) in patients with moderate-to-severe AD; and patients who
have already completed treatment will be followed up in the Long-Term Extension
(LTE) study (NCT07003425).
Bosakitug (previously ATI-045 or BSI-045B) was
in-licensed by Aclaris Therapeutics from Biosion and is a high-affinity
humanized anti-thymic stromal lymphopoietin (TSLP) antibody (over 150-fold
higher in vitro efficacy compared to tezepelumab) and an extremely low
dissociation rate from TSLP leading to long residence time and enhanced
neutralization activity and a half-life that can potentially support a dosing
interval of every 2 weeks. Aclaris’ Chinese partner Chia Tai Tianqing
(CTTQ) has already advanced bosakitug into phase 3 trials for severe asthma and
chronic rhinosinusitis with nasal polyps.
In the phase 2a Proof-of-Concept (POC) trial
(NCT05932654, ADAMANT), 300 mg bosakitug (BSI-045B) SC injections through 23
weeks were able to achieve significant improvements in efficacy measures at
week 23 (79% of the AD subjects achieved an IGA 0/1,
89% achieved an EASI-75, 44% achieved an EASI-90 and 28% achieved an EASI-100)
and a good safety profile87. A
further phase 2 trial (NCT07011706) is now
investigating the efficacy and safety of repeated SC injections of ATI-045 or
placebo administered to approximately 90 adult patients with moderate-to-severe
AD. The primary endpoint is percent change from baseline in EASI at week 24.
Secondary endpoints at week 24 include EASI50/75/90 responses, vIGA
response, BSA response and PP-NRS score, relative to baseline. Top-line results
are expected in the second half of 2026.
GIA632
from Novartis is a humanized IgG1 monoclonal
antibody that selectively binds to interleukin-15 (IL-15) and potently inhibits
its activity. IL-15 belongs to the common γ-chain (γc) family of
cytokines and is produced by monocytes/macrophages and dendritic cells, as well
as by stromal cells in tissues such as epithelium. The target cells for IL-15
are mainly lymphocytes and eosinophils. Intracellular IL-15 signal transduction
involves the JAK1/3-STAT3/5 pathway and drives co-stimulatory signals to effector
cytotoxic T cells. This way Il-15 promotes tissue protection by the elimination
of infected cells. Chronically overexpression of IL-15 in tissues may however
trigger the development of T cell-mediated disorders associated with tissue
destruction88. Although
IL-15 is mostly associated with type 1 (and not type 2) immunity, it has been
proposed as a therapeutic target as significant IL-15 overexpression was found
in AD skin lesions as well as in AD skin suction blisters89,90.
A recent genome-wide association study (GWAS) using cell-type enrichment confirmed the known pathobiology
of T-cell driven inflammation in AD involving TH1, TH2, TH17 and Treg cell
dysregulations7.
GIA632
is currently investigated in a phase 2a trial (NCT07220577) to assess its
efficacy (IGA response at week 16 defined as clear (0) or almost clear (1)
score with at least a 2 point-reduction from baseline), safety and tolerability
compared to placebo in approximately 84 adult patients with moderate to severe
atopic dermatitis.
Galvokimig (UCB9741) from UCB Biopharma is a
multi-specific antibody targeting IL-13, IL-17A and IL-17F with an extended
half-life through albumin binding. It is designed to selectively inhibit two
distinct and separate inflammatory pathways, TH2 (via IL-13) and TH17 pathways
(via IL-17A/F), that are involved in the chronic inflammation in AD. Positive data were obtained in a two-part, randomized,
first-in-human, proof-of-concept, double-blind Phase 1/2a single dose study of
galvokimig, where 47 patients with moderate to severe AD received one
intravenous injection of galvokimig (n=33) or placebo (n=14)91. At Week 12, a median of 64.9% of
patients achieved EASI-75 with galvokimig versus 12.3% with placebo. In
addition, a median of 46.6% of patients achieved EASI-90 with galvokimig versus
3.5% with placebo at week 12. In
December 2025, the phase 2b dose-ranging trial (NCT07277660) was
initiated to investigate the efficacy, safety, pharmacokinetics and
pharmacodynamics of galvokimig in adult patients with moderate to severe AD.
Participants will receive a predefined galvokimig dose or placebo during
initial intervention period. After week 16 participants will continue on the
same or a modified dose of galvokimig. The primary endpoint is the EASI-75 at
week 16.
Temtokibart (LEO 138559) from LEO
Pharma is a monoclonal antibody targeting IL22 receptor subunit alpha 1
(IL22RA1), a receptor for the proinflammatory cytokine IL-22 primarily
associated with TH17 and TH22 cell responses. Binding IL‑22 to the receptor
activates JAK1 and TYK2, which further phosphorylate and activate STATs (STAT1,
STAT3 or STAT5) which are responsible for a broad spectrum of downstream
effects92. Increased IL-22 levels are observed in patients with AD and
contribute to the manifestation of its characteristic symptoms. Elevated
IL-22 levels in patients with AD correlate with increased proliferation of
keratinocytes, alterations in the skin microbiota and impaired epidermal
barrier function93,94. At the EADV 2025 Congress, topline data from the phase 2b
trial (NCT05923099) evaluating temtokibart in adults with moderate to severe AD
were presented. Temtokibart was well tolerated and significantly reduced EASI
scores at week 16 for the 3 highest doses: 300 mg (-64.3%; P <
.01), 450 mg (-57.1%; P < .05) and 600 mg (-61.2%; P <
.01). The placebo group showed a mean EASI reduction of −41.7%. EASI improvements were generally maintained up to week
32, indicating potentially durable effects of temtokibart in a subset of
patients95 (Figure 10). Temtokibart
was well-tolerated with no dose-dependent AEs, low incidence of conjunctivitis
and no signal for herpes. In addition, reductions in EASI and SCORAD
scores correlated strongly with reductions in TH2, TH17 and TH22 cytokine
signatures and improvements in quality-of-life metrics (Dermatology Life
Quality Index and Patient-Oriented Eczema Measure)96.
Figure 10: EASI changes under temtokibart or placebo
from baseline to week 16 and up to week 3295.

12. Regulatory T cell (Treg) Proliferators
Regulatory T cells (Tregs)
account for 5-10 % of the peripheral blood CD4+ cells showing the
constitutive co-expression of CD25 (also known as the IL-2 receptor alpha).
Treg include two main subpopulations: natural Treg (nTreg) expressing the
nuclear transcription factor–forkhead winged helix P3 (FoxP3) and inducible
Treg which differentiate from nTreg after stimulation with IL-10 (T-regulatory
type 1 cells, Tr1) or TGF-ß (Th3/TH2 cells). Treg may express many other
receptors including the cytotoxic T lymphocyte-associated protein 4 (CTLA4),
the glucocorticoid-induced tumor necrosis factor receptor-related protein
(GITR), L-selectin (CD62L) and OX40 (CD134). Due to different expressions of
these receptors, Treg modulate the function of other cells not only in the
peripheral blood but also in the skin97,98.
Treg are important modulators of immune responses and able to suppress allergic
sensitization and immune responses driven by inflammatory TH1, TH2, TH17 and B
cells via several major pathways. In addition, Treg have direct and indirect
suppressive effects on mast cells, basophils and eosinophils99. Thus, stimulation of Treg proliferation
seems to be a promising approach to down-regulate the inflammatory process in
skin allergic reaction.
The Treg proliferation
stimulator REZPEG (rezpegaldesleukin) from Nektar
Therapeutics entered already phase 2 of clinical development for AD. REZPEG is
a pegylated-recombinant-human IL-2 that was recently evaluated in the phase 2b REZOLVE-AD
trial (NCT06136741) for its efficacy and safety in 393 adult patients with
moderate to severe AD. Key enrolment criteria in the study included a
minimum EASI score of 16.0, a minimum BSA of 10% and a minimum
vIGA-AD of 3. Patients were randomized (3:3:3:2) to receive treatment with
three SC doses of REZPEG (a high dose of 24 µg/kg every two weeks, a middle
dose of 18 µg/kg every two weeks and a low dose of 24 µg/kg every four weeks or
placebo every two weeks). The trial met its primary endpoint of the mean
improvement in Eczema Area and Severity Score (EASI) from baseline at week 16
for all three dose arms of REZPEG versus placebo (p<0.001). All three dose
arms also achieved statistical significance at week 16 for the key secondary
endpoints of EASI-75, EASI-50 and BSA100 (Table 5). In addition, blood biomarker
data demonstrate on-target and dose-dependent pharmacological activity with an
increase in total Tregs of up to 6-fold in the high dose arm. Sustained Treg
cell proliferation was observed at week 16 as compared to baseline and was
correlated with reduction of key TH2 inflammatory markers: IL-19, TARC (Thymus
and activation-regulated chemokine - also known as CCL17), periostin and
MDC/CCL22.
Table 5: Primary endpoint and key secondary endpoint data of
the phase 2b REZOLVE-AD trial.
|
|
REZPEG 24 µg/kg q2w (high dose) |
REZPEG 18 µg/kg q2w (middle dose) |
REZPEG 24 µg/kg q4w (low dose) |
Placebo |
|
Primary Endpoint |
N=104 |
N=106 |
N=110 |
N=73 |
|
Mean improvement in EASI score
from baseline |
61% p<0.001 |
58% p<0.001 |
53% p<0.001 |
31 % |
|
Key Secondary |
|
|
|
|
|
EASI-75 |
42% p<0.001 |
46% p<0.001 |
34% p<0.05 |
17 % |
|
EASI-50 |
66% p<0.001 |
66% p<0.001 |
55% p<0.01 |
34 % |
|
Mean improvement in BSA score from baseline |
54% p<0.001 |
48% p<0.001 |
43% p<0.001 |
17 % |
|
vIGA-AD 0/1 |
20% p<0.05 |
26% p<0.01 |
19% ns |
8 % |
|
EASI-90 |
25% p<0.05 |
18% ns |
17% ns |
9 % |
|
Itch NRS* |
42% p<0.01 |
35% p<0.05 |
23% ns |
16 % |
*Patients with baseline
Itch NRS ≥ 4 used as denominator for assessing Itch NRS response (N=63, 95, 92
and 102 for the placebo, 24 µg/kg q2w, 18 µg/kg q2w and 24 µg/kg q4w arms);
ns=not significant100.
13. Kinase Inhibitors
ICP-332 from Beijing
InnoCare Pharma is an oral highly potent and selective TYK2 inhibitor. By
acting on the TYK2 kinase domain (JH1), ICP-332 inhibits the activity of
inflammatory cytokines, such as IL-23, IL-12, IFN-α and IFN-β and thereby, it
inhibits pathways involved in the pathogenesis of AD. ICP-332 has already
entered phase 3 (NCT06775860) of clinical development due to the positive phase
2 results in patients with moderate to severe AD, in which once daily doses of
ICP-332 80 mg or 120 mg compared to placebo resulted in significant reductions
in EASI scores from baseline to week 4 combined with a good safety profile101.
Soquelitinib (CPI-818)
from Corvus Therapeutics is an oral selective inhibitor of IL-2 inducible T
cell kinase (ITK), an enzyme that is expressed predominantly in T cells and
plays a role in T cell activation and differentiation. Soquelitinib has been
shown to and induce the generation of Th1 helper cells while blocking the
development of both Th2 and Th17 cells and production of their secreted
cytokines. Th2 and Th17 helper T cells are involved in the pathogenesis of many
autoimmune and allergic diseases including AD. In addition, soquelitinib has
demonstrated anti-tumor activity in vivo in several syngeneic murine tumor
models and may represent a novel approach to cancer immunotherapy102. Soquelitinib has already demonstrated
positive safety and efficacy results in a phase 1 trial (NCT06345404) in
moderate to severe AD patients,
who have received prior systemic therapy including patients who were treatment
resistant103. Based on these data, a first phase 2 trial (NCT07441395)
is currently evaluating soquelitinib in patients with moderate to severe atopic
dermatitis that have failed at least one prior topical or systemic therapy.
Furthermore, due to positive results of a phase 1b clinical trial in patients
with refractory T cell lymphomas, which demonstrated tumor responses in very
advanced, refractory, difficult to treat T cell malignancies, a phase 3 registration
trial (NCT06561048) investigates the safety and efficacy of soquelitinib
in patients with relapsed/refractory peripheral T cell lymphoma.
ATI-2138 from Aclaris
Therapeutics is an oral dual inhibitor of the IL-2 inducible T cell kinase (ITK)
and JAK3 blocking T cell activation and proinflammatory cytokine signalling in
atopic skin. ITK regulates T cell receptor signal transduction and inhibition
of this kinase can affect T cell differentiation and activation. JAK3 is a key
signal transduction kinase that forms a heterodimer with JAK1, modulates JAK1
phosphorylation of STAT5 and regulates cytokines that signal through the IL-2
receptor common gamma chain (IL-2ϒc) to affect lymphocyte proliferation and
activation. A small phase 2a open-label clinical trial (NCT06585202) investigated
ATI-2138 administered over 12 weeks to participants with moderate to severe AD.
Twelve patients completed the study and data from 9 per protocol patients were
evaluated. The trial has demonstrated potential AT-2138 efficacy (77.1 % mean
improvement in EASI score at week 12). About 62.5 % of patients experienced at
least a 4-point improvement of the PPNRS. The safety profile was good (no
severe adverse events). Pharmacodynamic analyses demonstrated modulation of
both the ITK and JAK3 pathways. Near-complete (~95%) ITK target occupancy was
observed at peak, with 60-70% persisting at trough. Immunophenotyping of whole
blood showed no significant perturbation in T cells or NK cells. Proteome and
transcriptome tape strip and biopsy analyses of lesioned skin showed
significant reduction of multiple inflammatory markers with downregulation of
key ITK-dependent pathways (Th2, Th17, TCR and T-cell activation), along with
reduction in fibrosis-related markers and changes in epidermal barrier genes
suggesting restoration of skin homeostasis. Nevertheless, the current dose of
10 mg was considered low, suggesting higher doses may be needed in a larger
phase 2 trial104,105.
Barzolvolimab
(CDX-0159) from Celldex Therapeutics is a humanized IgG1k monoclonal antibody that binds the extracellular
domain of the receptor tyrosine kinase KIT (c-KIT/CD117) with high specificity
and sub-nanomolar affinity and allosterically inhibits activation by its only
ligand Stem Cell Factor (SCF). Modifications to the Fc fragment of
barzolvolimab eliminated FcγR binding and the potential for significant
infusion-related reactions through Fc-mediated mast cell activation and
enhanced antibody serum exposure in non-human primates. KIT is highly expressed
in mast cells, which are important immune sentinel cells but increased mast
cell activity is involved in allergies, inflammation and pruritus, the key
drivers of AD.
Inhibition of KIT/SCF
by barzolvolimab reduces mast cell differentiation, maturation and survival. Barzolvolimab
has shown a good safety profile and target-engagement through suppression of
plasma tryptase (a marker of tissue mast cell numbers) in healthy human
subjects supporting its potential utility in mast cell-driven disorders106. Barzolvolimab is currently tested in a phase 2 trial
(NCT06727552) in patients with moderate to severe AD will receive barzolvolimab
by SC injections of 150 mg or 300 mg (after an initial loading dose of 450 mg)
or placebo every 4 weeks followed by a re-randomized crossover treatment
regimen for further 16 weeks. The primary endpoint is the percent change
from Baseline in the weekly average of the daily worst-itch (PP-NRS) score at
Week 16.
CGB-500 (ointment of
tofacitinib) from CAGE Bio is a novel ionic
liquid–based topical therapy of the pan-JAK inhibitor tofacitinib in
development for patients with atopic dermatitis. In 2025, positive results from
a phase 2b dose-ranging study of CGB-500 (NCT06810050) have been
announced demonstrating efficacy, rapid itch relief and a favourable safety
profile in AD patients with moderate to severe disease affecting less than 10%
of BSA107. Approximately 59% of patients achieved clear or almost
clear skin with at least a two-grade improvement of IGA and 71% of patients
achieved at least a 4-point reduction on the PP-NRS scale. About 35% of
patients reported a “0” itch score, indicating complete resolution of itch
symptoms. CGB-500 was generally well tolerated with no new or unexpected safety
concerns identified in the trial.
MH004 (tofacitinib
etocomil) 1.0% ointment from Minghui Pharmaceutical is a twice-daily pan-Jak
inhibitor, for which positive results were obtained
in a phase 3 trial (NCT07185282) in adolescents (ages 12 years and older) and
adults with mild to moderate AD. Both primary endpoints (IGA of clear or almost
clear with a 2-grade improvement and EASI75) were met at week 4: 41.0% of
individuals treated with MH004 1.0% achieved IGA-TS compared to 10.3%
treated with vehicle (P<0.0001 and 58.2% of individuals treated with MH004
1.0% achieving EASI-75 compared to 19.8% treated with vehicle (P<0.0001).
Additionally, the key secondary endpoints, including IGA-TS and EASI-75 at
week 8, as well as the proportion of participants with a ≥ 4-point improvement
in Itch Numerical Rating Scale (NRS4) score at week 8, were met. MH004 1.0% was
safe and well-tolerated108.
LNK01004 from
LYNK Pharmaceuticals is a topical pan-JAK inhibitor, showed significant
efficacy in treating moderate-to-severe atopic dermatitis in a phase 2 trial (NCT07071610)109. At week 8, both
concentrations of LNK01004 demonstrated superior efficacy compared with
vehicle, with the most pronounced responses observed in patients with higher
baseline BSA involvement. Among patients with BSA ≥10%, EASI-75 response rates
were 61.1% for the 0.3% group and 46.2% for the 1.0% group, compared with 20%
for vehicle. Similarly, vIGA-AD response rates (0/1 with ≥2-point improvement)
were 44.4% and 38.5% for the 0.3% and 1.0% groups, respectively, versus 10% for
vehicle. LNK01004 was well tolerated, with no treatment-related serious adverse
events reported. All treatment-related adverse events were mild or moderate
(Grade 1–2). Pharmacokinetic analyses revealed low systemic exposure, with mean
Cmax values of 0.06 ng/mL for the 0.3% dose and 0.15 ng/mL for the 1.0% dose.
14. STAT 6 Degrader
Targeting STAT6 directly may represent a new approach to
therapeutically modulate JAK–STAT signalling in AD and related allergic
conditions110,111. STAT6 (Signal
Transducer and Activator of Transcription 6) is an essential transcription
factor in the IL-4 and IL-13 signalling pathways and the central driver of TH2 immune
responses, including IgE class switching, eosinophil recruitment, mucus
production and expression of inflammatory mediators such as eotaxin (CCL11) and
TARC (CCL17)112. Multiple gain of
function mutations of STAT6 were identified to cause severe allergic diseases
in humans113. Dupilumab, an
injectable monoclonal antibody that blocks IL-4/13 signalling, is an approved
therapy for multiple allergic diseases. STAT6 targeting is therefore supported
by both human genetics and dupilumab’s clinical pathway validation114.
KT-621 from Kymera Therapeutics is a first-in-class
highly potent oral STAT6 degrader that can selectively degrade and deplete
STAT6 in various disease relevant human immune and tissue cells, fully block
various IL-4/13 functions in these cells with picomolar IC50 lower than the
IL-4Rα monoclonal antibody dupilumab and does not degrade or inhibit any other
STAT transcription factors. In a MC903-induced atopic dermatitis mouse model orally
administered KT-621 demonstrated complete inhibition on the total serum IgE, a
TH2 inflammation biomarker114 (Figure 11). In the phase 1b BROADEN trial (NCT06945458), KT-621 (100 mg and 200 mg
once daily oral treatment for 28 days) showed significant STAT6 degradation in
blood and skin, indicating effective target engagement in AD patients. In addition,
a reduction in type 2 inflammatory biomarkers (similar to IL4/IL-13 blockage)
and relevant improvements on clinical endpoints (EASI-75 improvement from
baseline was 33% and 25% in the 100 mg and 200 mg dose groups, respectively)
and patient-reported outcomes were reported which need to be confirmed in
larger trials. KT-621 was reported to be well tolerated with no unexpected
safety issues or dose-limiting toxicities reported, though detailed adverse
event data have not yet been released115. KT-621 is currently in Phase 2 clinical testing - a
Phase 2 BROADEN2 trial (NCT07217015) started in November 2025 in moderate to
severe AD patients with data expected to be reported by mid-2027. It is a
16-week double-blind, placebo-controlled study with a 52-week open-label period
and intended to enable dose selection for subsequent parallel phase 3 trials in
AD.
Figure 11: KT-321 inhibits IL-4 and IL-13 signalling pathways
and Th2 Inflammation in AD114.
15. Other
Zabalafin hydrogel from Alphyn Biologics is a
non-steroidal, topical AD treatment containing multiple bioactive (undisclosed)
components which are directly targeting the bacteria living on the skin of
patients with AD. Bacteria like Staphylococcus aureus naturally live on the
skin and discharge toxins that make AD symptoms worse and often cause infection
and prevent healing. In a phase
2a trial, about 90% of
patients experienced a 1-point reduction in IGA score and a Patient Oriented
Eczema Measure (POEMA) scale quality-of-life improvement of at least 6 by the
end of treatment with zabalafin 9.5% gel. Additionally, 68% of patients
experienced an itch score improvement of at least 4 on the PP-NRS with 84% of
patients with infected skin reaching complete clearance. All patients also had
a decrease in Skin Infection Rating Scale (SIRS) score with only 1
reported treatment-emergent adverse event of mild transient stinging116. A phase 2b trial (NCT06855745, CLEAR-AD1) is currently testing the
efficacy, safety and tolerability of a 9.5 % zabalafin gel compared to vehicle
for 4 months in 72 patients with mild to moderate AD.
Based on a thorough review of the clinical trial
projects currently in phase 2 and phase 3 published on CLINICALTRIALS.GOV and
the publicly available literature, the current drug candidates for topical and
systemic administration are summarised in (Table 6 and Table 7),
respectively.
Table 6: Currently most advanced AD drug candidates for topical administration.
|
Product / Sponsor |
Target/ Route of administration |
Development Phase/NTC (clinialtrials.gov) |
|
JAK Inhibitors |
||
|
MH004 (tofacitinib etocomil) / Minghui Pharmaceutical |
Novel 1% ointment of tofacitinib |
Phase 3: NCT07185282 Completed in AUG-2025 |
|
CGB-500 / CAGE Bio |
Novel ionic liquid–based ointment of tofacitinib |
Phase 2b: NCT06810050 Completed 2025, positive results announced SEP-2025 |
|
LNK01004
/ LYNK Pharmac. |
Topical pan-JAK inhibitor |
Phase 2 trial: NCT07071610 Completed 2025, positive results announced NOV-2025 |
|
Other |
||
|
Zabalafin gel / Alphyn Biologics |
Multiple bioactive components targeting bacteria living on AD skin |
Phase 2: NCT06855745 (CLEAR-AD1) Recruiting, SCE: NOV-2025 |
|
Abbreviations: JAK = Janus kinase, SCE = Study completion estimated |
||
Source: Data in public domain on ClinicalTrails.gov
Table 7: Currently most advanced AD drug candidates for systemic administration.
|
Product / Sponsor |
Target/ Route of administration |
Development Phase/NTC (clinialtrials.gov) |
|
Monoclonal antibodies targeting inflammatory
cytokine signalling |
||
|
APG 777 / Apogee Therapeutics |
High-affinity anti-IL-13 mAb with extended half-life
for SC injection |
Phase 2: NCT06395948 Recruiting, SCE: JUN-2028 NCT07003425 (LTE of NCT06395948), Recruiting, SCE: DEC-2029 |
|
Bosakitug (ATI-045, previously BSI-045B) / Aclaris Therapeutics |
High-affinity
humanized anti-TSLP antibody (over 150-fold higher in vitro efficacy compared
to Tezepelumab) for SC injection |
Phase 2: NCT07011706 Active,
Not Recruiting, SCE: OCT-2026
|
|
GIA632/ Novartis |
Humanised anti-IL15 mAb for
SC administration |
Phase 2a: NCT07220577 Recruiting, SCE: Sep 2027 |
|
Galvokimig (UCB9741) / UCB Biopharma |
Bispecific antibody targeting IL-13, IL-17A, IL-17F
for IV and SC injection |
Phase 2: NCT07277660 Recruiting, SCE: MAR-2028 |
|
Temtokibart (LEO 138559) / LEO Pharma |
Anti-IL-22 mAb |
Phase 2b: NCT05923099 |
|
Monoclonal antibodies targeting OX40/OX40L pathway |
||
|
Amlitelimab (SAR445229) / Sanofi
|
Fully human anti-OX40L IgG4 mAb for SC
administration |
Phase 3: ESTUARY (NCT06407934) Ongoing to confirm and extend the findings of COAST
1 (NCT06130566),
COAST 2 (NCT06181435) and SHORE (NCT06224348) |
|
Telazorlimab (ISB 830) / Ichnos Sciences SA |
Humanized anti-OX40 IgG1 for SC administration |
Phase 2b: NCT03568162 Completed AUG 2021 |
|
IMG-007 / Inmagene
LLC
|
anti-OX40 mAb engineered to silence ADCC function for SC injection |
Phase 2b: NCT07037901 (ADAPTIVE) Recruiting, SCE: OCT-2027 |
|
Treg proliferators |
||
|
REZPEG (rezpegaldesleukin)/ Nektar Therapeutics
|
Pegylated-recombinant-human IL-2 for SC
administration |
Phase 2b: NCT06136741 (REZOLVE-AD) Long-term maintenance phase ongoing |
|
Kinase Inhibitors |
||
|
ICP-332 / Beijing InnoCare Pharma |
Oral TYK2 inhibitor |
Phase 3: NCT06775860 Recruiting, SCE: DEC-2026 |
|
ATI-2138 / Aclaris Therapeutics |
Oral dual inhibitor of ITK and JAK3 |
Phase 2: NCT06585202Completed MAR-2025 |
|
Barzolvolimab (CDX-0159) / Celldex Therapeutics |
Humanized anti- KIT mAb for SC administration |
Phase 2: NCT06727552 Recruiting, SCE: May-2027 |
|
Soquelitinib (CPI-818)
/ Corvus Pharmaceuticals |
Oral ITK inhibitor |
Phase 2: NCT07441395 Recruiting,
SCE: SEP-2027 |
|
STAT 6 Degrader |
||
|
KT-621 / Kymera Thrapeutics |
Oral STAT 6 degrader
|
Phase 2: NCT07217015 |
|
Abbreviations: ADCC = antibody-dependent
cellular cytotoxicity, AhR = aryl hydrocarbon receptor, ITK = IL-2 inducible
T cell kinase, JAK = Janus kinase, KIT = CD117,
LTE = long-term-extension; mAb = monoclonal antibody, SC = subcutaneous, SCE = Study completion estimated,
SYK = Spleen tyrosine kinase, TYK2 = Tyrosine kinase 2. |
||
Source: Data in public domain on ClinicalTrails.gov
16. Concluding Remarks
Managing atopic dermatitis is complex and often faces challenges such as treatment resistance, medication adherence or identifying triggers. Individual therapy needs to be tailored to patient needs and disease severity. The ideal outcome in AD patients would be no itch, no rash and no adverse effects. A big step in this direction was the approval of monoclonal antibodies targeting TH2 immune responses such as dupilumab, tralokinumab, lebrikizumab and recently also nemolizumab. This has encouraged the development of small compounds targeting the TH2 interleukin IL-4/IL-13 pathway, such as JAK inhibitors, which can be taken orally and work fast to relieve symptoms, particularly itching. Unlike monoclonal antibodies that target only one or two specific cytokines, JAK-inhibitors block multiple signalling pathways at once, making them highly effective against a wide range of inflammatory signals in AD. This comprehensive blockade, however, can affect essential immune functions, which may lead to side effects like an increased risk of severe infection. In addition, FDA still requires black box warnings about an increased risk of serious heart-related events, cancer, blood clots and death for the class of JAK inhibitors. In this regard, long-term comparative efficacy and safety data are still missing in the literature. Some new topical therapies have recently reached the US and Japanese market including novel JAK inhibitors (ruxolitinib, delgocitinib), phosphodiesterase 4 (PDE4) inhibitors (crisaborole, difamilast, roflumilast) and the aryl hydrocarbon receptor agonist tapinarof. New innovative approaches for systemic therapy are thought to adopt better individual patient needs and requirements including lower dosing frequency and less side effects. Most advanced new drug developments are monoclonal antibodies targeting the OX40/OX40L pathway, such as amlitelimab and the oral TYK2 inhibitor ICP-332 for systemic administration. Novel promising topical therapies include ointments of pan-JAK inhibitors, such as MH004, CGB-500 and LNK01004 and the antimicrobial gel zabalafin.
17. References
- Langan SM, Irvine AD, Weidinger S. Atopic
Dermatitis. Lancet, 2020;396: 345-360.
- Tian J, Zhang D, Yang Yet
al. Global epidemiology of atopic dermatitis: a comprehensive systematic
analysis and modelling study. Br J Dermatol, 2023: 1-7.
- Skayem
C, Richard MA, Aroman MS, et al. Epidemiology of atopic dermatitis: a global
worldwide study. Clin Exp Dermatol, 2025;50: 2054-2056.
- Lambrecht BN and Hammad H. The immunology of the allergy epidemic
and the hygiene hypothesis. Nature Immunology, 2017;18(10).
- Gallagher K, Halperin-Goldstein S, Paller AS. New
treatments in atopic dermatitis update. Ann
Allergy Asthma Immunol, 2025;135: 498-510.
- Croft M, Esfandiari E, Chong C, et al. OX40 in the pathogenesis of atopic
dermatitis-a new therapeutic target. Am J Clin Dermatol, 2024;25(3): 447-461.
- Oliva M, Sarkar MK, March ME et al. Integration
of GWAS, QTLs and keratinocyte functional assays reveal molecular mechanisms of
atopic dermatitis. Nature Communications, 2025;16: 3101.
- Suresh MS,
Kaliyadan F.
Assessing eczema severity: A comprehensive review of scoring systems.
Indian Journal of Skin Allergy, 2025;4(1): 19-24.
- Yosipovitch G, Reaney M, Mastey V, et al. Peak
Pruritus Numerical Rating Scale: psychometric validation and responder
definition for assessing itch in moderate-to-severe atopic dermatitis. Br
J Dermatol, 2019;181(4): 761-769.
- Wollenberg A, Kinberger M, Arents B, et al. European Guideline (EUROGUIDERM) on atopic eczema:
Living update. J Eur Acad Dermatol Venereol, 2025;39: 1537-1566.
- Davis DMR, Frazer-Green L, Alikhan A et al. Focused update: Guidelines of care for the management of atopic
dermatitis in adults. J Am Acad Dermatol, 2025;93(3):745.
- https://www.jaad.org/article/S0190-9622(26)00343-9/fulltext
- Wichmann K, Uter W, Weiss J et
al. Isolation of
alpha-toxin-producing Staphylococcus aureus from the skin of highly sensitized
adult patients with severe atopic dermatitis. Br J Dermatol, 2009;161(2):
300-305.
- Adviti T,
Almsallaty
N, Chalati T, et al. Role of methicillin-resistant Staphylococcus aureus in cutaneous infections: Current
treatments and therapeutic approaches for future advancement. International
Journal of Pharmaceutics, 2025;684: 126030.
- Hülpüsch C, Rohayem R, Reiger M, et al. Exploring
the skin microbiome in atopic dermatitis pathogenesis and disease modification.
J Allergy Clin Immunol, 2024;154(1): 31-41.
- Jaffary F, Faghihi G, Mokhtarian A, et al.
Effects of oral vitamin E on treatment of atopic dermatitis: A randomized controlled
trial. J. Res. Med. Sci, 2015;20: 1053-1057.
- Nielsen AY, Høj S, Thomsen SF, et al. Vitamin D
supplementation for treating atopic dermatitis in children and adults: A
systematic review and meta-analysis. Nutrients, 2024;16: 4128.
- Bath-Hextall
FJ, Jenkinson
C, Humphreys R, et al. Dietary supplements for established atopic eczema. Cochrane Database Syst Rev, 2012;(2): d005205.
- Harb H, Chatila TA. Mechanisms of Dupilumab. Clin Exp Allergy, 2020;50: 5-14.
- https://www.google.com/url?sa=t&rct=j&q=&esrc=s&source=web&cd=&ved=2ahUKEwjRvaqZ18uQAxXOQfEDHTG0IEsQFnoECCIQAQ&url=https%3A%2F%2Fwww.ema.europa.eu%2Fen%2Fdocuments%2Fproduct-information%2Fdupixent-epar-product-information_en.pdf&usg=AOvVaw1kRThmMsc9lKbTJoQZUxdJ&opi=89978449
- Simpson EL, Bieber T, Guttman-Yassky E et al. Two Phase 3 Trials of Dupilumab versus
Placebo in Atopic Dermatitis. N Engl J Med, 2016;375: 2335-2348.
- Worm M, Simpson EL, Thaci D, et al. Efficacy and Safety of Multiple
Dupilumab Dose Regimens After Initial Successful Treatment in Patients with
Atopic Dermatitis: A Randomized Clinical Trial. JAMA Dermatol, 2020;156:
131-143.
- Zirwas M,
Chovatija R, Stein Gold L, et al. Conjunctivitis adverse events in dupilumab
clinical trials. British Journal of Dermatology, 2024;190(2): 58-59.
- Zhao ZY, Zhang L, Wu L, et al. Long-term
efficacy and safety of stapokibart for moderate-to severe atopic dermatitis.
Allergy, 2025;80: 1348-1357.
- Shi Y, Ho M, Li H, Collazo R, et al.
Optimized second-generation IL-4Rα inhibition: structural and molecular
dynamics properties of rademikibart Fab-IL-4Rα complex. Poster presented at:
Fall Clinical Dermatology Conference.
- Zhang J, Silverberg JI, Li P, et al. CBP-201, a
next-generation IL-4Rα antibody, achieved all primary and secondary efficacy
endpoints, with a favorable safety profile, in adults with moderate-to-severe
atopic dermatitis (AD): A randomized, double-blind, pivotal trial in China
(CBP-201-CN002). Oral presentation #45874, 2023 Annual Meeting of the American
Academy of Dermatology (AAD 2023); New Orleans, LA, USA.
- Silverberg JI, Strober B, Feinstein B, et al. Efficacy and safety of rademikibart
(CBP-201), a next-generation monoclonal antibody targeting IL-4Rα, in adults
with moderate-to-severe atopic dermatitis: a phase 2 randomized trial
(CBP-201-WW001). J Allergy
Clin Immunol, 2024:153(4): 1040-1049.
- Zhang J, Silverberg JI, Guo J, et
al. Positive 52-Week Maintenance Data Observed with
Rademikibart in Patients with Moderate-to-Severe Atopic Dermatitis (SEASIDE
CHINA) RAD, 2024.
- Tollenaere MAX, Mølck C,
Henderson I, et al. Tralokinumab Effectively Disrupts the IL-13/IL-13Ra1/IL-4Ra
Signalling Complex but Not the IL-13/IL-13Ra2 Complex. JID Innovations, 2023;3:
100214.
- Wollenberg A, Blauvelt A,
Guttman-Yassky E, et al. Tralokinumab for moderate‐to‐severe atopic dermatitis:
results from two 52‐week, randomized, double‐blind, multicentre, placebo‐controlled
phase III trials (ECZTRA 1 and ECZTRA 2). Br J Dermatol, 2021;184: 437-449.
- Silverberg JI, Toth D,
Bieber T et al. Tralokinumab plus
topical corticosteroids for the treatment of moderate-to-severe atopic dermatitis: results from the double-blind, randomized,
multicentre, placebo-controlled phase III ECZTRA 3 trial. Br J Dermatol.
2021;184: 450-63.
- https://www.google.com/url?sa=t&rct=j&q=&esrc=s&source=web&cd=&ved=2ahUKEwiElvCV28uQAxVLBNsEHaXUJJsQFnoECAsQAQ&url=https%3A%2F%2Fwww.ema.europa.eu%2Fen%2Fdocuments%2Fproduct-information%2Febglyss-epar-product-information_en.pdf&usg=AOvVaw3F6uiPRFaqLZncEV8Z91HS&opi=89978449
- https://www.ema.europa.eu/en/medicines/human/EPAR/ebglyss
- Guttman-Yassky E, Irvine A, Simpson E, et al.
Long-term efficacy and safety of lebrikizumab is maintained in patients with
moderate-to-severe atopic dermatitis: results up to 3 years from ADjoin.
Presented at: Society for Pediatric Dermatology Annual Meeting, 2025.
- Hermanns
HM. Oncostatin M and interleukin-31: cytokines, receptors, signal transduction
and physiology. Cytokine Growth Factor Rev 2015, 26(5): 545-58.
- Sonkoly
E, Muller A, Lauerma A, et al. IL-31: a new link between T cells and pruritus
in atopic skin inflammation. J Allergy Clin Immunol, 2006;117(2): 411-417.
- Cevikbas F, Wang X, Akiyama T, et al. A sensory neuron–expressed IL-31 receptor mediates T helper
cell–dependent itch: involvement of TRPV1 and TRPA1. J Allergy Clin Immunol,
2014;133(2): 448-460.
- Singh B,
Jegga AG, Shanmukhappa KS, et al. IL-31 driven skin
remodeling involves epidermal cell proliferation and thickening that lead to
impaired skin-barrier function. PLoS One, 2016;11(8): e0161877
- Silverberg JI, Wollenberg A, Reich A,
et al. Nemolizumab with concomitant topical therapy in
adolescents and adults with moderate-to-severe atopic dermatitis (ARCADIA 1
& 2): results from two replicate, double-blind, randomised controlled phase
3 trials. Lancet. 2024.
- Augustin M, Tauber M, Sidbury
R et al. Safety and efficacy of nemolizumab for atopic
dermatitis up to 2 years in open-label extension study. J Eur Acad Dermatol Venereol, 2025.
- https://www.fda.gov/drugs/drug-safety-and-availability/fda-requires-warnings-about-increased-risk-serious-heart-related-events-cancer-blood-clots-and-death
- Mirali S, Drucker AM. New Topical and Systemic Treatments for Atopic Dermatitis. Clinical
& Experimental Allergy, 2025;55: 1057-1069.
- Reich K, Kabashima K, Peris K, et al. Efficacy and safety of baricitinib combined with
topical corticosteroids for treat-ment of moderate to severe atopic dermatitis:
a randomized clinical trial. JAMA Dermatol, 2020;156(12): 1333-1343.
- Bieber T, Katoh N, Simpson EL, et al. Safety of Baricitinib for the Treatment of Atopic Dermatitis Over a
Median of 1.6 Years and up to 3.9 Years of Treatment: An Updated Integrated
Analysis of Eight Clinical Trials, Journal of Dermatological Treatment, 2023;34(1):
2161812.
- Costanzo A, Torretto A, Simpson EL, et al. Safety of Baricitinib for the Treatment of Atopic Dermatitis in Adults Over
a Median of 1.6 and up to 4.6 Years Treatment: Final Integrated Analysis of
Eight Clinical Trials. JEADV Clinical Practice,
2026;5: 67-74.
- Silverberg JL, de Bruin-Weller M, Thaci D, et al. Efficacy and safety of abrocitinib in
adults and adolescents with moderate-to-severe atopic dermatitis (JADE-MONO-1).
Lancet, 2021;396(10255): 875-886
- Gooderham MJ, Forman SB, Bissonnette R, et al. Efficacy and safety of
Abrocitinib in patients with moderate to severe atopic dermatitis (JADE-MONO
2). JAMA Dermatol, 2020;156(6): 645-655.
- Bieber T, Simpson RS, Silverberg
JI, et al. Abrocitinib versus placebo or dupilumab for
atopic dermatitis. New English Journal of Medicine, 2021;384(12):
1102-1112.
- https://www.google.com/url?sa=t&rct=j&q=&esrc=s&source=web&cd=&ved=2ahUKEwj0k8iX3MuQAxVKRPEDHWuIF80QFnoECBsQAQ&url=https%3A%2F%2Fwww.ema.europa.eu%2Fen%2Fdocuments%2Fproduct-information%2Frinvoq-epar-product-information_en.pdf&usg=AOvVaw08Nx2FyfatQG7pnhdFtQBh&opi=89978449
- Sidbury R, Alikhan A, Bercovitch L, et al.
Guidelines of care for the management of atopic dermatitis in adults with
topical therapies. J
Am Acad Dermatol, 2023;89(1).
- Chaudhary F, Lee W, Escander T, et al. Exploring
the Complexities of Atopic Dermatitis: Pathophysiological Mechanisms and
Therapeutic Approaches. Journal of Biotechnology and Biomedicine, 7(2024):
314-328.
- Jacob SE, Steele T. Corticosteroid classes: a
quick reference guide including patch test substances and cross-reactivity. J
Am Acad Dermatol, 2006;54(4): 723-737.
- Stoughton RB. Bioassay system for formulations of
topically applied glucocorticosteroids. Arch Dermatol, 1972;106(6): 825-827.
- Niedner R. Therapie mit systemischen Glukokortikoiden. Hautarzt, 2001;52: 1062-71.
- https://iris.who.int/handle/10665/41975
- Luger T, Loske K D, Elsner P et al. Topische Dermatotherapie mit
Glukokortikoiden Therapeutischer Index. J Dtsch Dermatol Ges, 2004;2: 629-634.
- Schoepe S, Schäcke H, May E, et al.
Glucocorticoid therapy induced skin atrophy. Exp Dermatol, 2006;15: 406-420.
- Niedner R. Glukokortikosteroide in der Dermatologie: Kontrollierter
Einsatz erforderlich. Dtsch Arztebl International, 1996;93(44): 2868.
- Werfel T, Heratizadeh A, Aberer W, et
al. S3 Guideline Atopic dermatitis. AWMF-Registernr, 2023: 013-027.
- Kim
BS, Howell MD, Sun K, et
al. Treatment of atopic dermatitis with ruxolitinib cream (JAK1/JAK2
inhibitor) or triamcinolone cream. J Allergy Clin Immunol,
2020;145: 572-582.
- AAAAI/ACAAI JTF Atopic Dermatitis Guideline
Panel, Chu DK, Schneider L, et al. Atopic dermatitis (eczema) guidelines: 2023
American Academy of Allergy, Asthma and Immunology/American College of Allergy,
Asthma and Immunology Joint Task Force on Practice Parameters GRADE-and
Institute of Medicine-based recommendations. Ann Allergy Asthma Immunol, 2024;132: 274-312.
- Ghanem
L, Mendoza- Millán DL, Lopes BB, et al. Ruxolitinib cream improves outcomes in
atopic dermatitis: An updated systematic review and meta- analysis. Pediatr
Allergy Immunol, 2026;37: e70281.
- Nakagawa
H, Nemoto O, Igarashi A, et
al. Delgocitinib ointment, a topical Janus kinase inhibitor, in adult
patients with moderate to severe atopic dermatitis: a phase 3, randomized,
double-blind, vehicle-controlled study and an open-label, long-term extension
study. J Am Acad Dermatol, 2020;82: 823-831.
- Nakagawa H, Igarashi A, Saeki
H, et al. Safety, efficacy and pharmacokinetics of delgocitinib ointment in
infants with atopic dermatitis: A phase 3, open-label and long-term study. Allergology International, 2024;73: 137e142.
- Bissonnette
R,
Warren RB,
Pinter A, et al. Efficacy and safety of delgocitinib cream in adults with moderate to
severe chronic hand eczema (DELTA 1 and DELTA 2): results from multicentre,
randomised, controlled, double-blind, phase 3 trials. Lancet, 2024;404(10451):
461-473.
- Gooderham M, Molin S,
Bissonnette R, et al. Long-term safety and efficacy of delgocitinib cream
for up to 52 weeks in adults with Chronic Hand Eczema: Results of the phase 3
open-label extension DELTA 3 trial following the DELTA 1 and 2 trials. J Am Acad Dermatol, 2025;11.
- https://www.ema.europa.eu/de/documents/product-information/anzupgo-epar-product-information_de.pdf
- Blauvelt A,
Langley RG, Gordon KB, et al. Next Generation PDE4 Inhibitors that Selectively
Target PDE4B/D Subtypes: A Narrative Review. Dermatol Ther (Heidelb), 2023;13: 3031-3042.
- Paller AS, Tom WL, Lebwohl
MG, et al. Efficacy and safety of crisaborole ointment, a novel, nonsteroidal
phosphodiesterase 4 (PDE4) inhibitor for the topical treatment of atopic
dermatitis (AD) in children and adults. J Am Acad Dermatol, 2016;75(3): 494-503.
- Hiyama H, Arichika N, Okada
M, et al. Pharmacological Profile of Difamilast, a Novel Selective
Phosphodiesterase 4 Inhibitor, for Topical Treatment of Atopic Dermatitis. J
Pharmacol Exp Ther, 2023;386: 45-55.
- Saeki H,
Ito K, Yokota D, et al. Difamilast ointment in adult patients with atopic
dermatitis: a phase 3 randomized double-blind vehicle-controlled trial. J Am
Acad Dermatol, 2021;86: 607-614.
- Saeki H,
Baba N, Ito K, et al. Difamilast, a selective phosphodiesterase 4 inhibitor,
ointment in paediatric patients with atopic dermatitis: a phase III randomised
double-blind, vehicle-controlled trial. Br J Dermatol, 2022;186: 40-49.
- Saeki H, Ohya Y, Baba N, et al. A Phase 3, Long‑Term, Open‑Label Study
of Difamilast Ointment to Evaluate Efficacy and Safety
in Japanese Infants with Atopic Dermatitis. Dermatol Ther, 2026;16: 339-352.
- Simpson E, Eichenfield L,
Geng B, et al. Pooled Efficacy,
Patient-reported Outcomes and Safety of Roflumilast Cream 0.15% from the
INTEGUMENT-1 and INTEGUMENT-2 Phase 3 Trials of Patients with Atopic Dermatitis
and Prior Inadequate Response, Intolerance and/or Contraindications for Topical
Corticosteroids. J Allergy Clin Immunol, 2025;155(2).
- https://www.accessdata.fda.gov/drugsatfda_docs/label/2025/215985s012lbl.pdf
- Arcutis Presents New Phase 2 Results in
Infants with Atopic Dermatitis in Late-Breaking Session Today at the 2026
American Academy of Dermatology Annual Meeting. Arcutis Presents New Phase 2 Results in Infants with
Atopic Dermatitis in Late-Breaking Session Today at the 2026 American Academy
of Dermatology Annual Meeting - Arcutis Biotherapeutics.
- Bissonnette R, Saint-CyrProulx E, Jack C, et al. Tapinarof for
psoriasis and atopic dermatitis: 15 years of clinical research. J EurAcad
Dermatol Venereol, 2023;37: 1168-1174.
- Silverberg J, Boguniewicz
M, Quintana FJ, et al. Tapinarof validates the aryl hydrocarbon receptor as a
therapeutic target: A clinical review. J Allergy Clin Immunol.
2024; Volume 154, Number 1, pages 1-10. https://doi.org/10.1016/j.jaci.2023.12.013
- https://www.accessdata.fda.gov/drugsatfda_docs/label/2024/215272s002lbl.pdf
- Valenzuela F, Meza V. 2025 Biologics:
Targets and Therapy. 2025;19: 281–288.
- https://pharmaphorum.com/news/sanofi-plans-amlitelimab-dermatitis-filing-after-new-readout
- Guttman-Yassky E, Simpson EL, Reich K, et
al. An anti-OX40 antibody to treat moderate-to-severe
atopic dermatitis: a multicentre, double-blind, placebo-controlled phase 2b
study. Lancet, 2023;401: 204-214.
- https://ir.kyowakirin.com/en/news/news-2560625228719159862/main/0/link/e20260303_01.pdf
- Rewerska B, Sher LD, Alpizar S,
et al. Phase 2b randomized trial of OX40 inhibitor telazorlimab for
moderate-to-severe atopic dermatitis. J Allergy Clin
Immunol Glob, 2024;3: 100195.
- Shen Y, Wu C, Nair A, et
al. Safety and Pharmacokinetics of IMG-007, an OX40 monoclonal antibody, in
healthy adults. Research Abstracts / Ann Allergy Asthma Immunol, 2023;131: 15-94.
- Rubio D, Zhu E, Thurston A, et al. Preclinical Safety of APG777, A
Novel Extended Half-Life Anti-Interleukin-13 Monoclonal Antibody, in Cynomolgus
Monkeys. International Journal of Toxicology,
2025;44(6): 443-450.
- Parish JL,
Appel JE, Silverberg JI, et al. Clinical
efficacy, safety and pharmacokinetic profile of bosakitug (BSI-045B), an
anti-thymic stromal lymphopoietin (TSLP) mAb in a phase 2 study of moderate and
severe atopic dermatitis subjects. British Journal of Dermatology, 2024;191(2).
- Jabri B, Abadie V. IL-15
functions as a danger signal to regulate tissue-resident T cells and tissue
destruction. Nat Rev Immunol, 2015;15(12): 771-783.
- Karlen H, Yousefi S, Simon HU, et al. IL-15
Expression Pattern in Atopic Dermatitis. Int Arch Allergy Immunol, 2020;181(6):
417-421.
- Rojahn TB, Vorstandlechner V,
Krausgruber T, et al. Single-cell transcriptomics
combined with interstitial fluid proteomics defines cell type-specific immune
regulation in atopic dermatitis. J Allergy Clin Immunol, 2020;146(5): 1056-1069.
- Hunter H, et
al. A
first-in-patient 18-week study of galvokimig, a multispecific antibody–based
therapeutic targeting interleukin (IL)-13, IL-17A and IL-17F in participants
with moderate-to-severe atopic dermatitis (AD).
- Laska J, Tota M, Łacwik J, et al.
IL‑22 in Atopic Dermatitis. Cells, 2024;13: 1398.
- Lou H, Lu J, Choi EB, et al.
Expression of IL‑22 in the Skin Causes Th2‑ Biased Immunity, Epidermal Barrier
Dysfunction and Pruritus via Stimulating Epithelial Th2 Cytokines and the GRP
Pathway. J Immunol, 2017;198: 2543-2555.
- Brunner PM, Pavel AB,
Khattri S, et al. Baseline IL-22 expression in patients with atopic dermatitis
stratifies tissue responses to fezakinumab. The Journal of Allergy and Clinical
Immunology, 2019;143(1): 142-154.
- Weidinger S, et al. IL-22RA1 antagonism
with temtokibart provides significant early and sustained improvements in
atopic dermatitis: results from a phase 2b dose finding trial. D1T01.E, EADV
Congress, 2025: 17-20.
- https://www.dermatologytimes.com/view/leo-pharma-presents-late-breaking-results-on-temtokibart-for-atopic-dermatitis-at-eadv
- Raimondi
G, Turner MS, Thomson AW, et al. Naturally occurring regulatory T cells:
recent insights in health and disease. Crit Rev Immunol, 2007;27: 61-95.
- Samochocki Z, Alifier M, Bodera P, et al. T-regulatory cells in severe
atopic dermatitis: alterations related to cytokines and other lymphocyte
subpopulations. Arch Dermatol Res, 2012;304:795-801.
- Palomares O, Yaman G, Azkur AK, et al. Role of Treg in
immune regulation of allergic diseases. Eur. J. Immunol, 2010;40: 1232-1240.
- https://ir.nektar.com/news-releases/news-release-details/rezolve-ad-phase-2b-study-rezpegaldesleukin-meets-primary-and
- Xu J, Zhang
L, Liang Y, et al. Safety and
Efficacy of ICP-332 for Moderate to Severe Atopic Dermatitis: A Phase 2
Randomized Clinical Trial. JAMADermatol, 2026;162(3): 227-235.
- Hsu
LH, Rosenbaum JT, Verner E et al. Synthesis and characterization of soquelitinib a selective ITK inhibitor
that modulates tumor immunity. npj Drug Discovery| (2024) 1:2.
- Corvus
Pharmaceuticals, Press Release, January 20, 2026. Corvus Pharmaceuticals Announces Positive
Data from Cohort 4 Confirming Results for Placebo-Controlled Phase 1 Clinical
Trial of Soquelitinib for Atopic Dermatitis. Corvus Pharmaceuticals
Announces Positive Data from Cohort 4 Confirming Results for Placebo-Controlled
Phase 1 Clinical Trial of Soquelitinib for Atopic Dermatitis | Corvus
Pharmaceuticals.
- https://seekingalpha.com/pr/20181712-aclaris-therapeutics-announces-positive-top-line-results-from-open-label-phase-2a-trial-of
- Aggarwal A, Kaul A, Stillwell L, et al.
Results from an Open-Label Phase 2 Trial of ATI-2138, an investigational oral
covalent inhibitor of interleukin-2-inducible T cell kinase (ITK) and Janus
kinase 3 (JAK3), in patients with moderate-to-severe atopic dermatitis.
American academy of Dermatology association. Poster ID: 74636.
- Alvarado D, Maurer M, Gedrich R, et al. The anti-KIT monoclonal antibody CDX- 0159
induces profound and durable mast cell suppression in a healthy
volunteer study. Allergy, 2022;77: 2393-2403.
- https://www.prnewswire.com/news-releases/cage-bio-reports-strong-results-from-its-phase-2b-atopic-dermatitis-trial-302547128.html?tc=eml_cleartime
- https://www.prnewswire.com/news-releases/minghui-pharmaceutical-announces-positive-topline-results-from-phase--trial-of-mh004-tofacitinib-etocomil-ointment-in-mild-to-moderate-atopic-dermatitis-302318768.html
- https://www.prnewswire.com/apac/news-releases/lynk-pharmaceuticals-announces-key-phase-ii-clinical-results-of-lnk01004-for-the-treatment-of-patients-with-moderate-to-severe-atopic-dermatitis-302618660.html
- Kolkhir P, Akdis CA, Akdis M,
et al. Type 2 Chronic Inflammatory Diseases: Targets,
Therapies and Unmet Needs. Nature Reviews. Drug Discovery, 2023;22: 743-767.
- Haikarainen T, Virtanen AT, Cravatt BF, et al. Pharmacological targeting
of the JAK–STAT pathway: new concepts and emerging indications. Nat Rev Drug Discov, 2026.
- Pfitzner E, Kliem S, Baus D, et al. The role of STATs in inflammation and inflammatory diseases. Curr Pharm
Des, 2004;10(23): 2839-2850.
- Sharma M, Leung D, Momenilandi M,
et al., Human germline heterozygous gain-of-function STAT6 variants cause
severe allergic disease. J Exp Med, 2023;220(5): 20221755
- Wang A, Yang B, Ramanathan
A, et al. Potent and Selective Oral STAT6 Degraders Inhibit IL-4 and IL-13
Functions in Human Cells and Block TH2 Inflammation in a Mouse Model of Atopic
Dermatitis. Annual Meeting American Academy of Dermatology, 2024.
- https://investors.kymeratx.com/news-releases/news-release-details/kymera-therapeutics-announces-positive-results-broaden-phase-1b
- https://www.prnewswire.com/news-releases/alphyn-announces-positive-results-from-second-cohort-of-phase-2a-clinical-trial-in-atopic-dermatitis-302082303.html
- Brockmöller J
and Tzvetkov MV. Pharmacogenetics: data, concepts and tools to improve drug
discovery and drug treatment. Eur J Clin Pharmacol, 2008;64: 133-157.
- https://www.google.com/url?sa=t&rct=j&q=&esrc=s&source=web&cd=&ved=2ahUKEwiZ_s-R2suQAxVFBdsEHbNCK_0QFnoECCYQAQ&url=https%3A%2F%2Fwww.ema.europa.eu%2Fen%2Fdocuments%2Fproduct-information%2Fadtralza-epar-product-information_en.pdf&usg=AOvVaw116d-6lXFDj-Z5QxJxUEQT&opi=89978449
- https://www.ema.europa.eu/en/documents/product-information/nemluvio-epar-product-information_en.pdf
- https://www.google.com/url?sa=t&rct=j&q=&esrc=s&source=web&cd=&ved=2ahUKEwiY9d_128uQAxUmQ_EDHenEFd4QFnoECAsQAQ&url=https%3A%2F%2Fwww.ema.europa.eu%2Fen%2Fdocuments%2Fproduct-information%2Folumiant-epar-product-information_en.pdf&usg=AOvVaw3LlZwyVzaFXGwji2W3nmMJ&opi=89978449
- https://www.google.com/url?sa=t&rct=j&q=&esrc=s&source=web&cd=&ved=2ahUKEwios4PD28uQAxUaXvEDHYxcAZkQFnoECAsQAQ&url=https%3A%2F%2Fwww.ema.europa.eu%2Fen%2Fdocuments%2Fproduct-information%2Fcibinqo-epar-product-information_en.pdf&usg=AOvVaw1HSdpNnAhjmWG2l35Q7ayH&opi=89978449
- https://www.accessdata.fda.gov/drugsatfda_docs/label/2025/215309s007lbl.pdf
- https://www.accessdata.fda.gov/drugsatfda_docs/label/2020/207695s007s009s010lbl.pdf
- https://www.accessdata.fda.gov/drugsatfda_docs/label/2026/219474Orig1s000lbl.pdf
- https://view.officeapps.live.com/op/view.aspx?src=https%3A%2F%2Fwww.rad-ar.or.jp%2Fsiori%2Fkusuri_sp_e%2F622784201_43533_nosp.doc&wdOrigin=BROWSELINK